New York State Workers' Compensation Board Forms
Documents:
627
This form is used to notify individuals in New York that they may be responsible for medical costs if their compensation claim is disallowed or if an agreement pursuant to Wcl 32 is approved. The form is available in both English and Spanish.
This document notifies you that you may be responsible for medical costs if your compensation claim is denied or if you fail to prosecute it. It is available in English and Chinese.
This form is used for notifying individuals that they may be responsible for medical costs if their compensation claim is not pursued, or if it is disallowed, or if an agreement under Wcl 32 is approved. It is available in English and Haitian Creole.
This form is used to notify individuals in New York that they may be responsible for medical costs if their compensation claim is disallowed or if an agreement according to WCL 32 is approved. It contains both English and Italian translations.
This form is used to notify individuals that they may be responsible for medical costs if their compensation claim is disallowed or if an agreement pursuant to WCL 32 is approved. The form is available in both English and Polish and is specific to the state of New York.
This Form is used for notifying individuals in New York that they may be responsible for medical costs if their compensation claim is disallowed or if an agreement pursuant to WCL 32 is approved. Available in English and Russian.
This form is used for modifying a previous report in the Alternative Dispute Resolution Program in New York.
This document is used for finalizing a dispute resolution or settlement claim through the Alternative Dispute Resolution Program in New York.
This form is used for reporting the findings of an examination or record review conducted by an impartial specialist in the state of New York.
This form is used for notifying workers in New York about their right to choose a healthcare provider authorized by the Workers' Compensation Board. It is available in English and Chinese.
This form is used for notifying workers in New York about their right to choose a healthcare provider authorized by the Workers' Compensation Board. The form is available in English and Haitian Creole languages.
This form is used for notifying workers in New York about their right to choose a healthcare provider authorized by the Workers' Compensation Board. The form is available in both English and Italian languages.
This form is used for notifying workers in New York about their right to choose a healthcare provider authorized by the Workers' Compensation Board. It is available in both English and Korean.
This form is used for informing workers in New York about their right to choose a healthcare provider authorized by the Workers' Compensation Board. The form is available in both English and Polish languages.
This Form is used for notifying workers in New York of their right to choose a healthcare provider authorized by the Workers' Compensation Board. It is available in both English and Russian languages.
This document is a form that allows for the limited release of health information in accordance with HIPAA regulations. It is specifically for use in New York and is available in Chinese.
This form is used for authorizing the limited release of health information according to HIPAA regulations in New York, translated into Haitian Creole.
This form is used as a continuation to the billing section of various other forms in New York for carriers/employers.
This form is used for ordering the Medical Treatment Guidelines in New York.
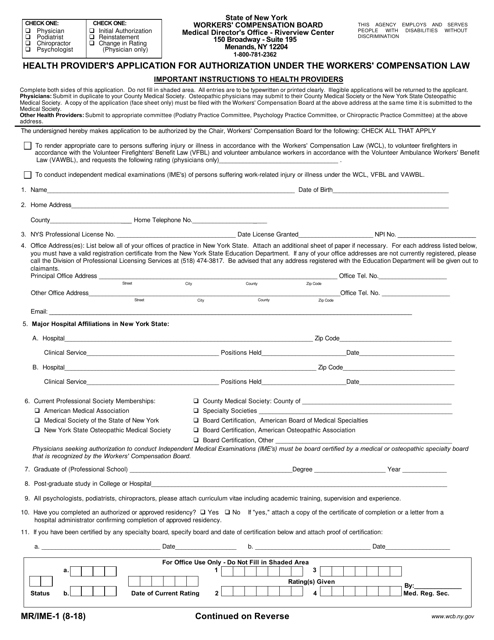
This Form is used for health providers in New York to apply for authorization under the Workers' Compensation Law.
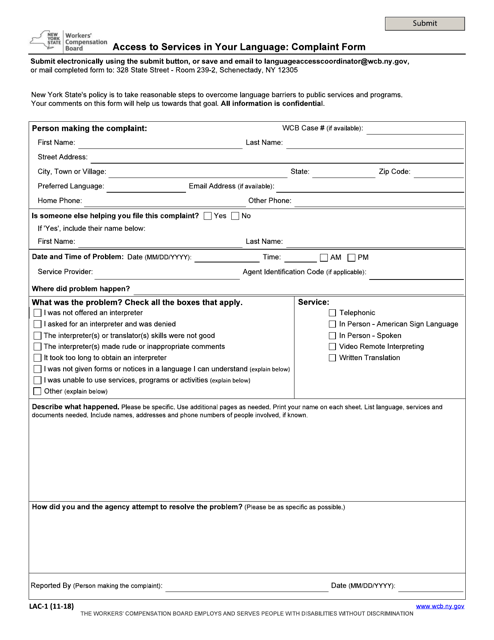
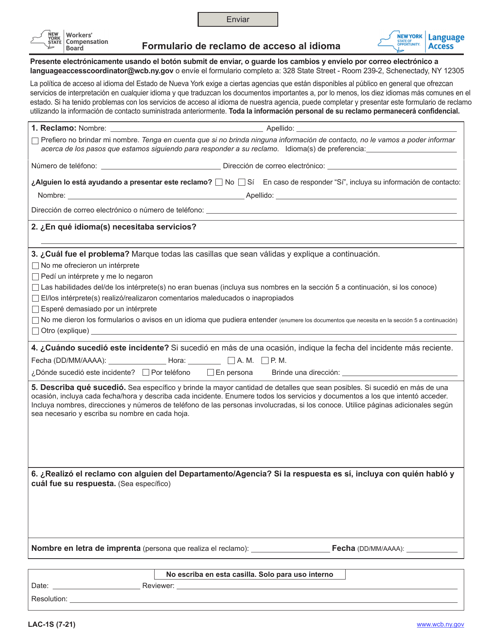
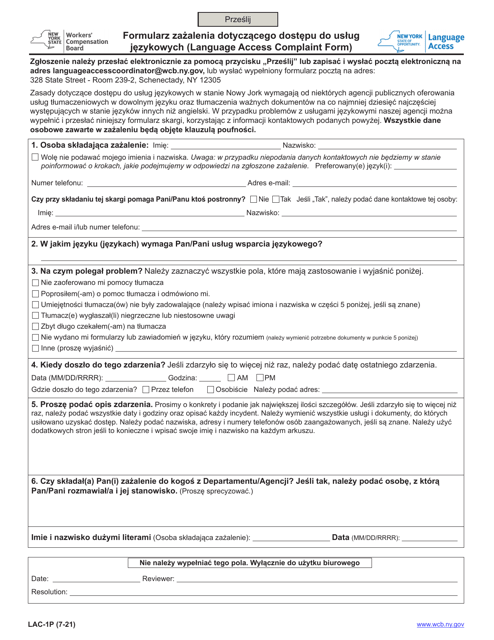
This form is used for lodging a complaint if you have faced difficulties accessing services in your preferred language in New York.
This form is used for filing complaints about access to services in Italian in the state of New York.
This form is used for filing a complaint about access to services in the Russian language in New York. It is designed to address any issues or concerns regarding language access in various services.
This Form is used for Disclosing Limited Health Information (HIPAA) - New York (Spanish).
This type of document is used for renouncing an agreement under Section 32 of the New York Workers' Compensation Law. (Note: This description is in English, but the form is in Spanish.)
This Form is used for requesting a redetermination due to extreme hardship in the state of New York.
This Form is used for registering independent job search efforts of applicants in New York.
This Form is used for employers in New York to report an illness or injury related to work. (Available only in Spanish)