Form CMS-10106 Authorization to Disclose Personal Health Information Release Form
What Is Form CMS-10106?
Form CMS-10106, 1-800-medicare Authorization to Disclosure Personal Health Information , is a formal document that lets Medicare beneficiaries authorize individuals or organizations they trust to examine their medical records and learn their protected health information. It is necessary to provide explicit permission to any person or company that requires access to your personal medical history, current treatment, and diagnosis. Additionally, you can handle the financial management of Medicare in case the authorized party must deal with the bills or debts.
Alternate Names:
- CMS Authorization Form;
- Medicare Form CMS-10106.
This form was issued by the Centers for Medicare & Medicaid Services (CMS) , a component of the U.S. Department of Health and Human Services . The latest version of the document was released on May 1, 2023 , with all previous editions obsolete. Download a CMS Authorization Form through the link below.
CMS Authorization Form Instructions
Follow these steps to prepare the CMS Authorization Form:
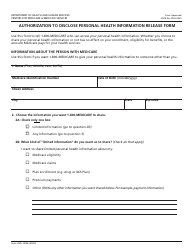
- State your full name, Medicare number from your Medicare card, and the birthdate.
- Check the appropriate box to confirm your intention to disclose all personal health details or only some of them - for instance, information about your claims, eligibility, or premiums to pay. Residents of New York State can exclude information about HIV, substance abuse, and mental health issues.
- Indicate the time period for the authorization - it may be indefinite or valid for a limited period. It is possible to revoke the authorization at any time.
- Provide the reason for the disclosure unless you prefer not to share this information.
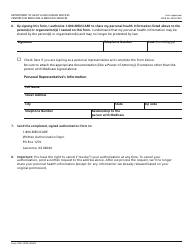
- Identify the person or organization who will be able to gain access to your personal health details by their name and address. You can add more than two people or companies on the back of the document.
- Certify your intention to share your health information by signing and dating the form. Write down your contact information. If the form is prepared by a person who already represents the patient in question, they must add their contact details as well and indicate their relationship to the beneficiary.
Download Form CMS-10106 Authorization to Disclose Personal Health Information Release Form

1
2

3
4

5

6