In Home Supportive Services Templates
Documents:
125
This form is used for notifying changes in the In-Home Supportive Services (IHSS) program in California. It notifies recipients of actions or decisions regarding their IHSS benefits.

This form is used for notifying individuals receiving In-Home Supportive Services (IHSS) in California about changes in their eligibility and continuation of services.
This form is used for notifying individuals in California about changes in their In-Home Supportive Services (IHSS) benefits. It serves as a notice of action regarding any modifications or adjustments to the IHSS program.
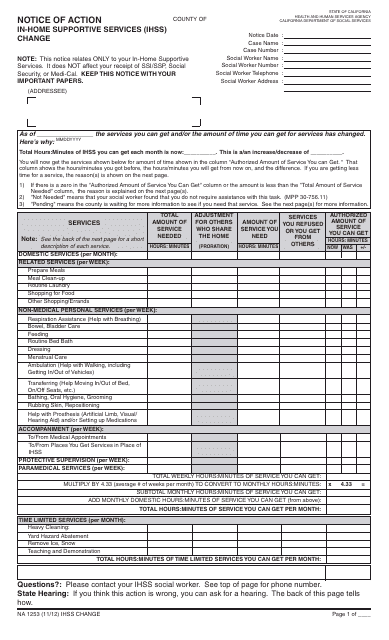
This form is used for notifying changes in the In-Home Supportive Services (IHSS) program in California.
This Form is used for notifying individuals in California who have been denied In-Home Supportive Services (IHSS). It provides information on the reasons for the denial and any steps that can be taken to appeal the decision.
This form is used for providing notice of action to inform individuals that their application for In-Home Supportive Services (IHSS) in California has been denied.
This form is used for the approval continuation of In-Home Supportive Services (IHSS) in California. It is a notice of action that informs individuals of the decision regarding their IHSS eligibility.

This form is used for notifying individuals in California about the approval continuation of In-Home Supportive Services (IHSS).
This form is used for notifying individuals in California about the approval of their In-Home Supportive Services (IHSS) application. It serves as a notice of action regarding their IHSS approval.
This Form is used for notifying the approval of In-Home Supportive Services (IHSS) in California.
This form is used for the In-Home Supportive Services (IHSS) Program in California. It informs the recipient that their provider's exemption from workweek limits is expiring.
This form is used for notifying providers in California's In-home Supportive Services Program that they are ineligible to request an exemption from workweek limits due to extraordinary circumstances.
This form is used for the In-Home Supportive Services (IHSS) program in California. It is a notice to inform providers that they have not received an exemption from the workweek limits specified in the Provider Agreement (APD 006).
This Form is used for notifying recipients of the In-Home Supportive Services (IHSS) program in California when their exemption from workweek limitations for extraordinary circumstances is discontinued.
This form is used for notifying providers of the In-Home Supportive Services (IHSS) program in California about the discontinuance of their exemption from workweek limitations due to extraordinary circumstances.
This form is used for changing the address and/or telephone number of providers or recipients in the In-Home Supportive Services (IHSS) Program in California.
This form is used for recipients of In-home Supportive Services in California to review and fulfill their responsibilities as employers of their home care workers.
This form is used for recipients of In-home Supportive Services (IHSS) in California to request the assignment of authorized hours to their providers.
This form is used for notifying the In-home Supportive Services Provider in California.
This form is used for the In-home Supportive Services (IHSS) Program in California to notify recipients about the requirement for health care certification.
This Form is used for notifying applicants/providers of the Incomplete Provider Process in the In-home Supportive Services Program in California.
Download this form, which is a medical certification submitted by a licensed health care professional to sanction the disabled, blind, or elderly access for services from the In-Home Supportive Services (IHSS) program.
This form is used for notifying the provider of violations for exceeding workweek and/or travel time limits in the In-Home Supportive Services Program in California.
This Form is used for notifying recipients of the approval of exemption from the in-Home Supportive Services Program workweek limits due to extraordinary circumstances in California's Ihss Program.
This form is used to notify the provider of the approval of an exemption from the in-Home Supportive Services (IHSS) program workweek limits for extraordinary circumstances in California.
This form is used for applying for an exemption from workweek limits for extraordinary circumstances under the In-Home Supportive Services program in California.
This document is for the In-Home Supportive Services (IHSS) Program in California. It is used for conducting a secondary evaluation of extraordinary circumstances.
This form is used for requesting exemption from workweek limits for extraordinary circumstances in the In-Home Supportive Services (IHSS) program in California.
This form is used for informing recipients that they are not eligible for exemption from the in-Home Supportive Services Program workweek limits due to extraordinary circumstances in California.
This form is used for applying for in-Home Supportive Services in California. It is the application form to request assistance with daily tasks for individuals who need support to live independently at home.
This form is used for applying for in-Home Supportive Services in California. It is designed to help individuals receive assistance and support with tasks such as personal care, household chores, and transportation.
This form is used for enrolling, changing, or cancelling direct deposit for In-Home Supportive Services (IHSS) and Waiver Personal Care Services (WPCS) providers in California.
This Form is used for notifying providers in the In-home Supportive Services Program in California about the third or fourth violation for exceeding workweek and/or travel time limits.
