California Department of Industrial Relations - Division of Workers' Compensation Forms
The California Department of Industrial Relations - Division of Workers' Compensation (DIR-DWC) is responsible for administering and enforcing the workers' compensation system in California. Its primary role is to ensure that injured workers receive appropriate medical treatment and benefits, while also facilitating the timely resolution of disputes related to workers' compensation claims. The DIR-DWC oversees various aspects of the workers' compensation process, including the regulation of qualified medical evaluators, monitoring medical provider networks, and providing resources and guidance to employers, employees, and insurance carriers.
Documents:
196
This document is used for submitting an application or plan for reapproval to the Medical Provider Network in California.
This Form is used for filing a Petition for Reconsideration with the California Division of Workers' Compensation Appeals Board (DWC/WCAB). It is a legal document used to request a review of a decision made in a workers' compensation case.
This Form is used for California QMEs to disclose their specified financial interests.
This Form is used for notifying the dismissal of an attorney in a workers' compensation case in California.
This document is used for submitting a declaration of service of a medical-legal report in California.
This form is used for submitting a voluntary directive for an alternate service of a medical-legal evaluation report on a disputed injury to the psyche in the state of California.
This form is used for applying for accreditation or re-accreditation as an education provider in California.
This form is used for declaring the protection of mental health records in California.
This document is a DWC Formulario 9768.10 which is used for requesting an Independent Medical Review in California.
This form is used for employees in California to complete a questionnaire regarding their disability status.
This document is used to request access to public records in the state of California.
This document is used for applying for a physician contract as an independent medical reviewer in California.
This Form is used for applying for an Independent Medical Review in California.
This document is used for notifying employees in California about injuries caused by work. It is available in both English and Spanish.
This form is used for requesting a Qualified Medical Evaluator (QME) panel under Labor Code Section 4062.2 in California.
This document is for filing a complaint about a Workers' Compensation Administrative Law Judge in California. It provides a formal process for addressing grievances or concerns regarding the judge's actions or decisions in workers' compensation cases.
This form is used for notifying the changes made to a Medical Provider Network Plan in California.
This form is used for reporting suspected medical care provider fraud in California.
This form is used for requesting accommodation by persons with disabilities in California.
This document is an application for Subsequent Injuries Fund benefits in the state of California. It is used by individuals who have suffered a subsequent injury and are seeking compensation and support from the Subsequent Injuries Fund.
This document is a request form used in California to initiate a dispute resolution process before the Administrative Director.
This form is used for healthcare providers in California to request a second bill review for a workers' compensation claim.
This document is used for notifying injured individuals in California of their options for regular, modified, or alternative work after an injury that occurred on or after January 1, 2013.
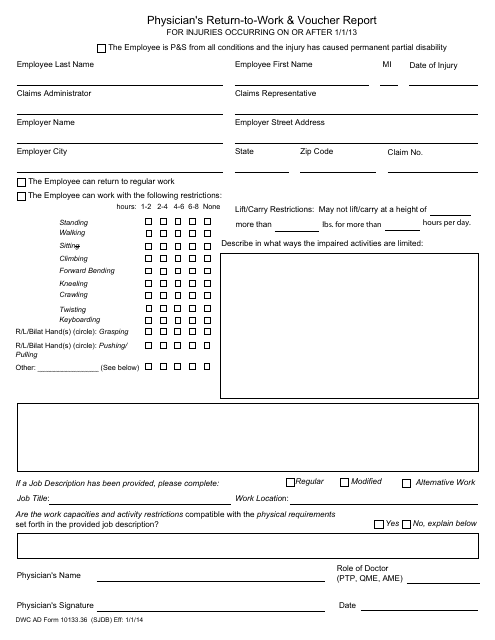
This form is used for reporting a physician's evaluation and recommendation for an individual's return to work in California, along with any necessary voucher information.
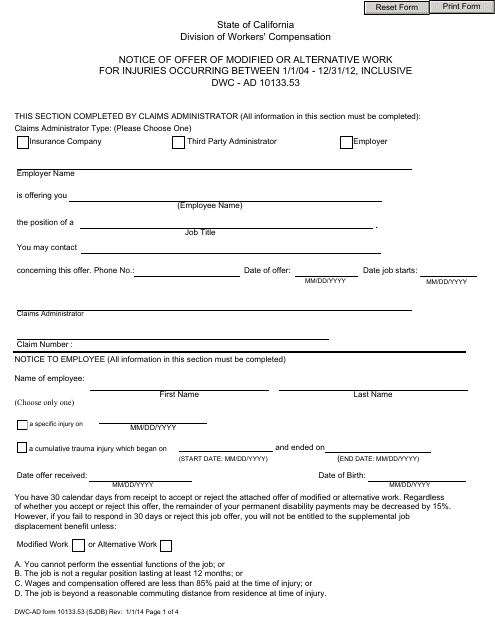
This document is used to notify injured workers in California about modified or alternative work options offered to them for injuries that occurred between 1/1/04 - 12/31/12.
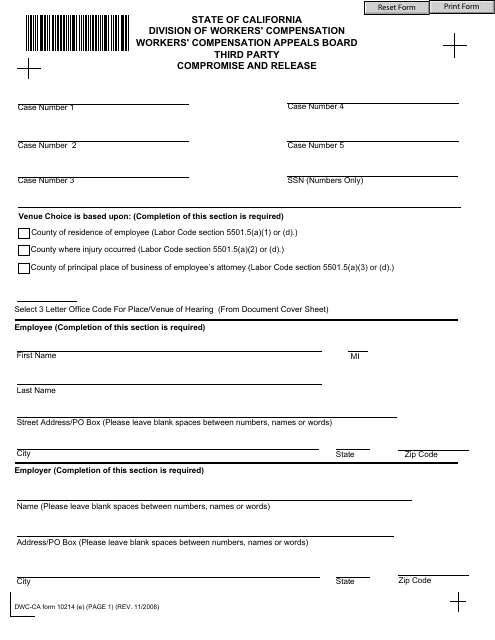
This form is used for settling a workers' compensation claim with a third party in California.
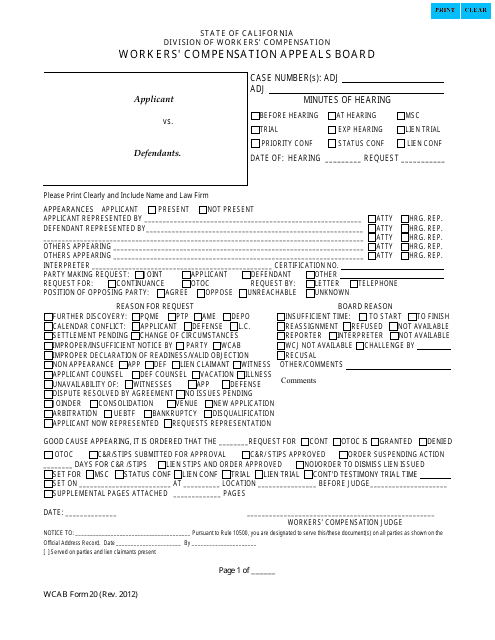
This form is used for recording the minutes of a hearing at the Workers' Compensation Appeals Board (WCAB) in California. It documents the proceedings, arguments, and decisions made during the hearing.
This form is used for notifying the California Division of Workers' Compensation (DWC) about having a personal chiropractor or personal acupuncturist.
This form is used for reporting employer payments in the state of California. It is used by employers to provide a statement of the payments made to their employees.
This form is used as a legal document and filled out by a treating physician of an employee with a work-related injury or illness to request authorization of special medical treatment, services, and procedures.
This document is used for reporting the progress of a patient's treatment by their primary treating physician in the state of California.
This Form is used for gathering information about an employee's permanent disability in California. It is a questionnaire that is specifically designed for Spanish-speaking individuals.
This form is used for faculty members in California to disclose any commercial interests they may have.
This document is used for disclosing any conflict of interest and waiving objections in relation to the QME or AME (Qualified/Agreed Medical Evaluator) process in California.
This Form is used for adding additional information to the Application for Adjudication of Claim form in California. It is specifically used to identify the legal entity that employs the injured worker.
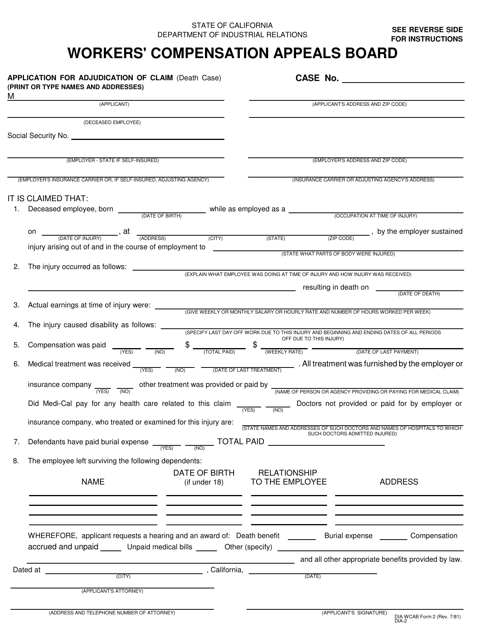
This type of document, called the DIA WCAB Form 2 (DIA2), is used in California for applying for the adjudication of a claim related to a death case.
This form is used for applying for discrimination benefits under Labor Code Section 132a in California. It is a verification form.

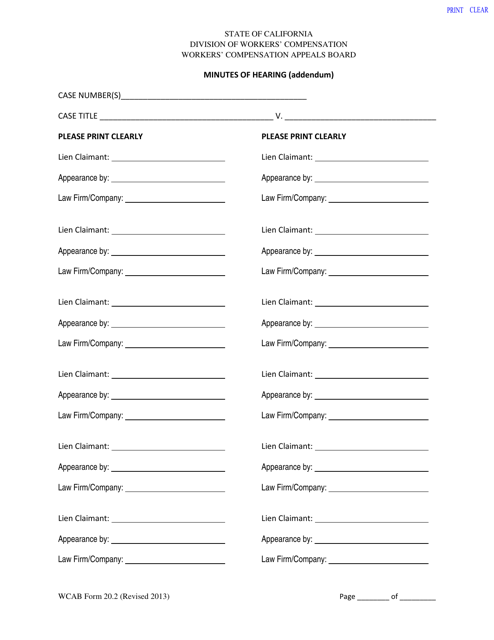
This document is used for recording additional minutes of a hearing in the state of California.
