Ohio Bureau of Workers' Compensation Forms
Documents:
289
This form is used for provider recertification in the state of Ohio. It is used by medical providers to apply for recertification to provide services to patients under the Ohio Bureau of Workers' Compensation.
This Form is used for submitting an amended true-up payroll report for Ohio. It is used to correct any errors or omissions in the original report.
This form is used for providers in Ohio to apply for enrollment in the Medical Managed Care Program, without needing to be certified.
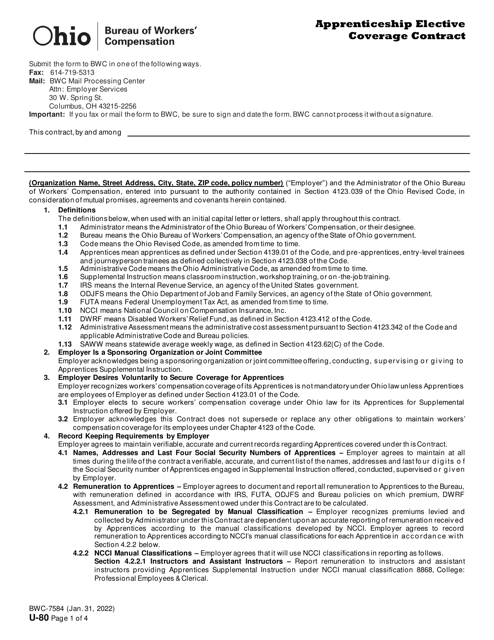
This Form is used for the Salary Continuation Agreement in the State of Ohio.
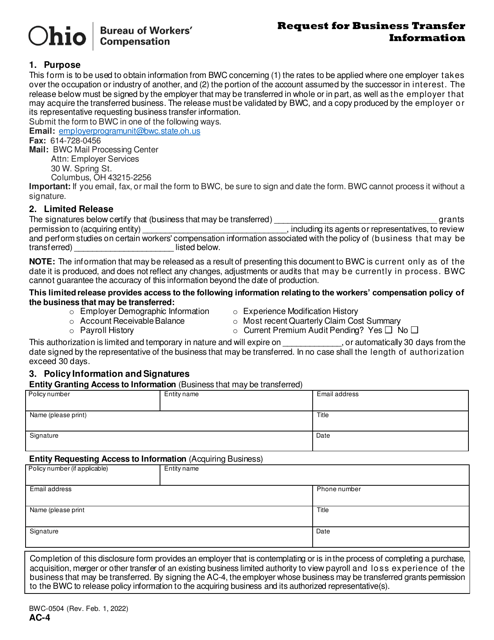
This Form is used for requesting the transfer of existing coverage from one employer to another in the state of Ohio.
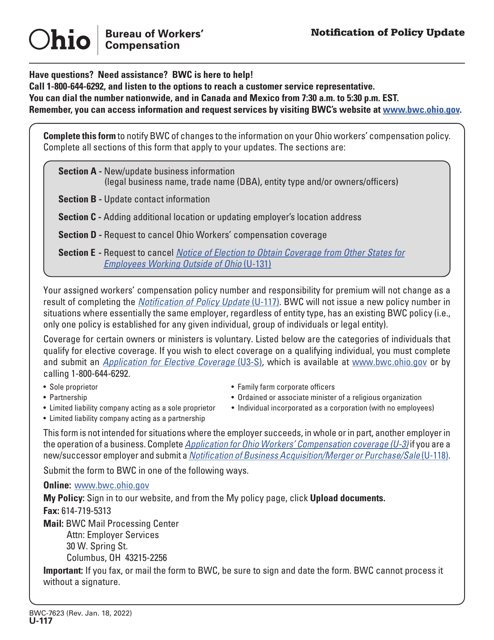
This form is used for notifying the Ohio Bureau of Workers' Compensation about adding or removing an additional named insured(s) on a policy.
This document is used for submitting a request to adjust the maximum allowable cost for medications in the state of Ohio.