![]() This version of the form is not currently in use and is provided for reference only. Download this version of
DD Form 2642
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
DD Form 2642
for the current year.
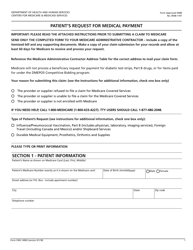
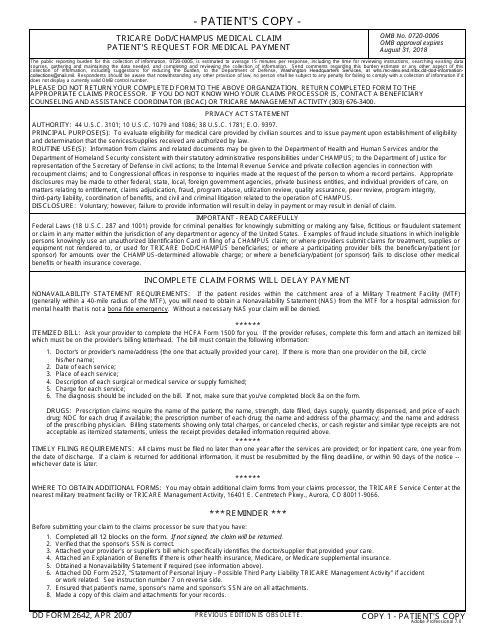
DD Form 2642 TRICARE DoD / CHAMPUS Medical Claim - Patient's Request for Medical Payment
What Is DD Form 2642?
DD Form 2642, TRICARE DoD/CHAMPUS Medical Claim - Patient's Request for Medical Payment also known as the Tricare DD Form 2642 is a form used for evaluating a service member's eligibility for medical care provided by civilian institutions.
This form - often incorrectly referred to as DA Form 264 - was revised by the Department of Defense (DoD) on April 1, 2007 . An up-to-date fillable DD Form 2642 is available for download and digital filing below or can be found on the Executive Services Directorate website.
The information from the claim may be released to the Department of Health and Human Services, the Department of Homeland Security, the Department of Justice, or other federal, state, local, or foreign agency upon legitimate request.
DD Form 2642 Instructions
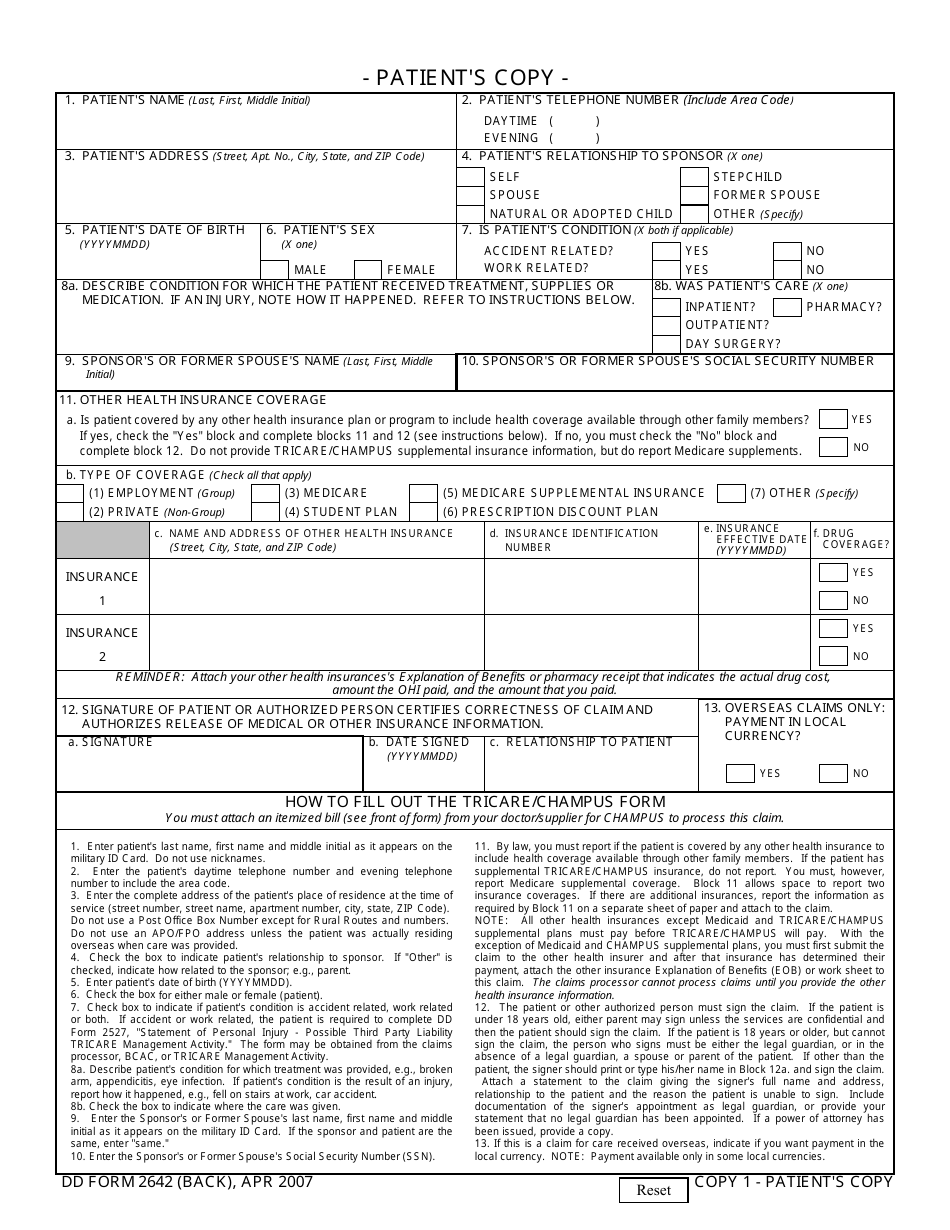
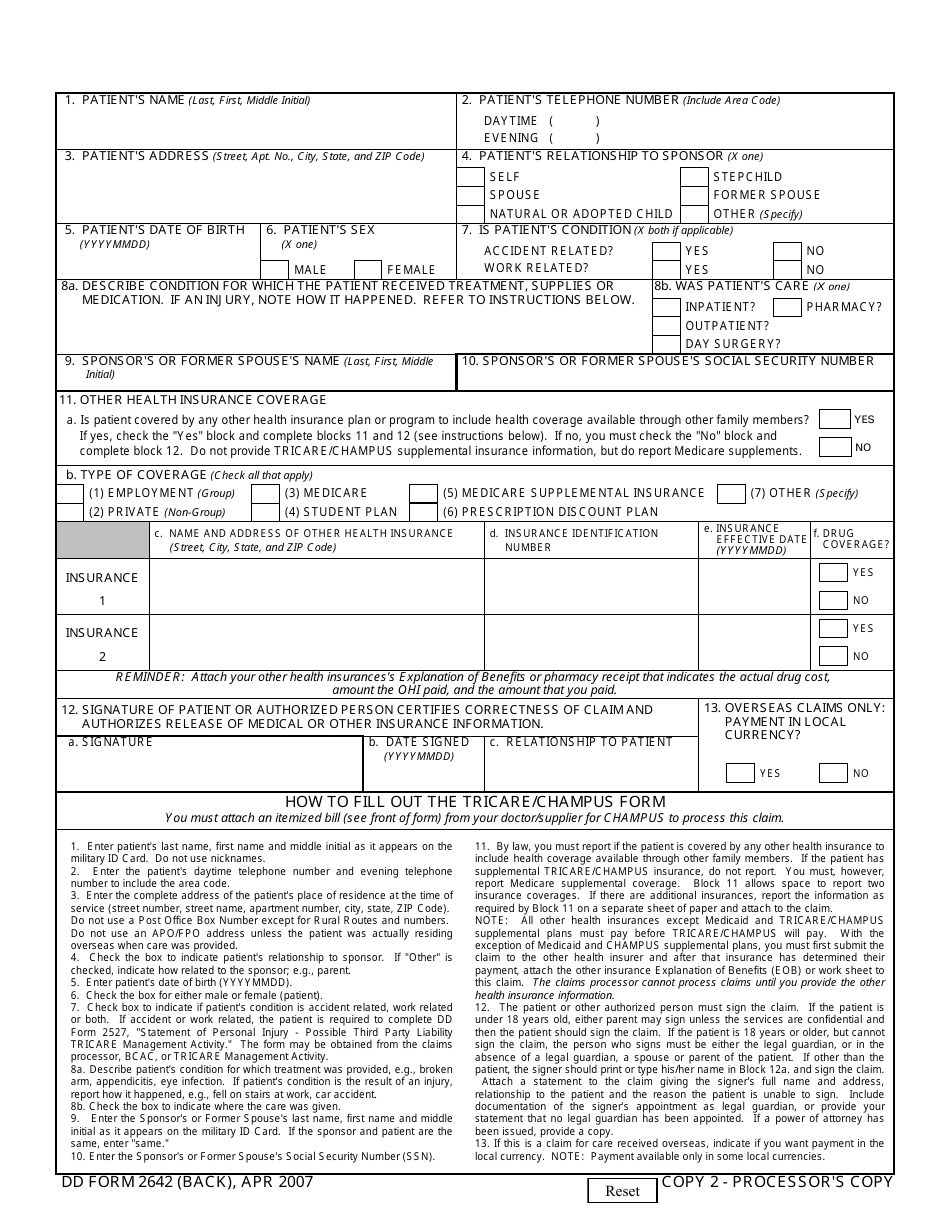
Usually, the provider fills the form and informs the receiver about the benefits. However, when a provider cannot file the form for a valid reason, the beneficiary has to file the claim themselves. The document consists of two copies. The patient keeps one and the other one is for a processor. Both copies must be completed.
- In order to submit the claims correctly and receive the answer in time, fill the form accurately and double-check the patients and the sponsor ID information.
- Fill the patients and sponsors personal information, state the patients' relation to the sponsor. If their condition is caused by accident or work-related, check the appropriate box. In these cases, the patient has to complete and attach DD Form 2527, Statement of Personal Injury.
- Describe the patients' condition and where it was treated.
- If the patient is covered by other health care insurance, including one received through other family members, this must be reported. However, TRICARE or CHAMPUS insurance should not be listed.
- Reporting the other coverage, provide full information on its name, address, identification number, effective date, and state if it covers drugs. Also, attach the Explanation of Benefits.
- The patient must sign and date the form. If the patient is under 18 or cannot sign the form, the legal representative must print their name in the signature block and sign the form.
- If care is required overseas, state if payment must be in local currency.
- Submit the DD 2642 Form with an itemized bill, an explanation of benefits, a nonavailability statement and a statement of personal Injury if these apply to your case.
The form and the attendant documents must be submitted within one year after the services are provided. For inpatient care, the deadline for the request is one year after hospital discharge date. If the document was returned for additional information, resubmit it within 90 days of the notice or by the filing deadline.
Where To Send DD Form 2642?
If care was received in the U.S. or the U.S territories and using TRICARE, send claims depending on the region you live in.
- For the West region send forms to the Claims Department, P.O. Box 202112, Florence, SC 29502-2112.
- For the East region mail forms to P.O. Box 7981, Madison, WI 53707-7981.
- If care was received outside of the U.S, send paperwork to claims departments of the institutions where you received the services. Or you can file them online using the TRICARE Overseas Beneficiary Portal.
- For care received through the CHCBP, send claims to the CHCBP claims processor.
Download DD Form 2642 TRICARE DoD / CHAMPUS Medical Claim - Patient's Request for Medical Payment
1
2

3
4