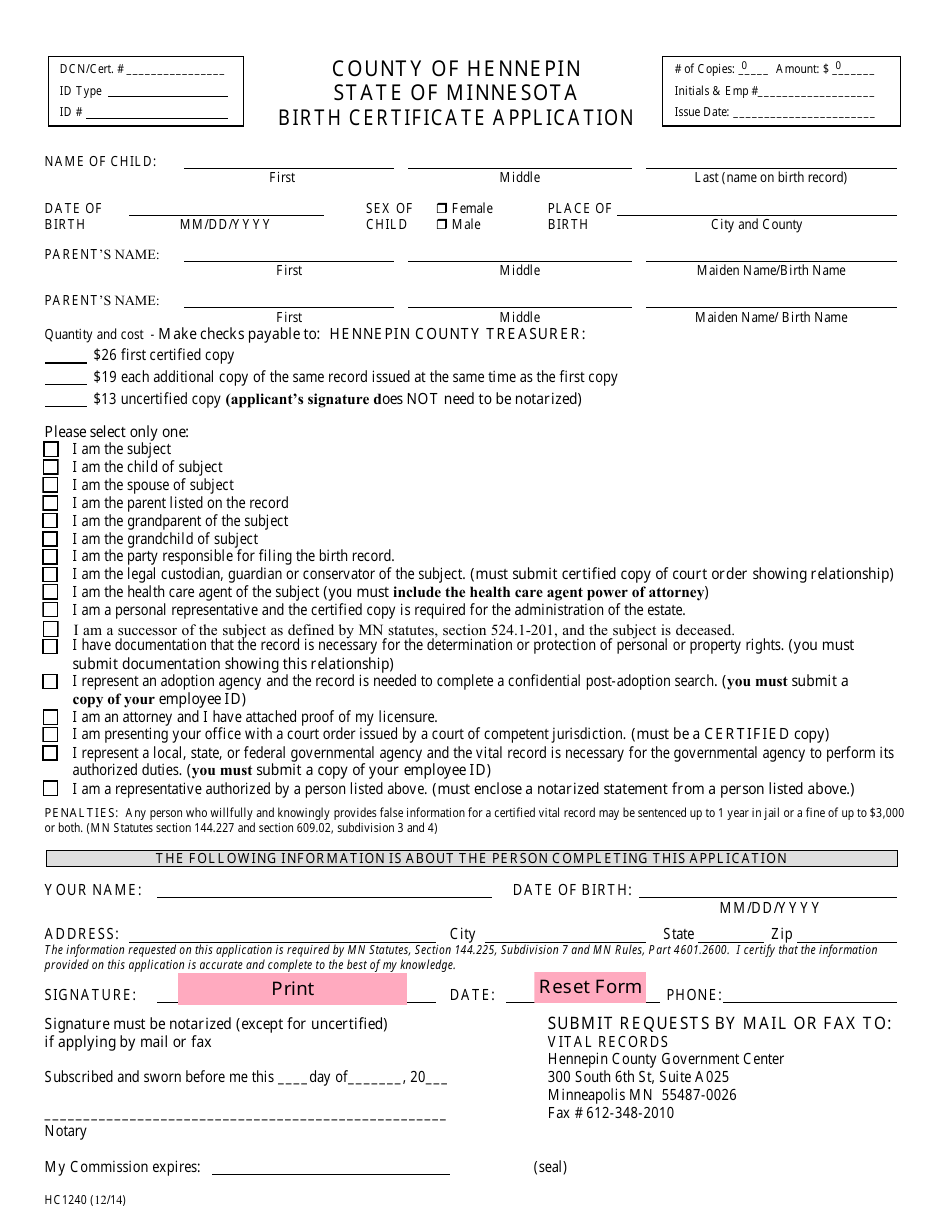
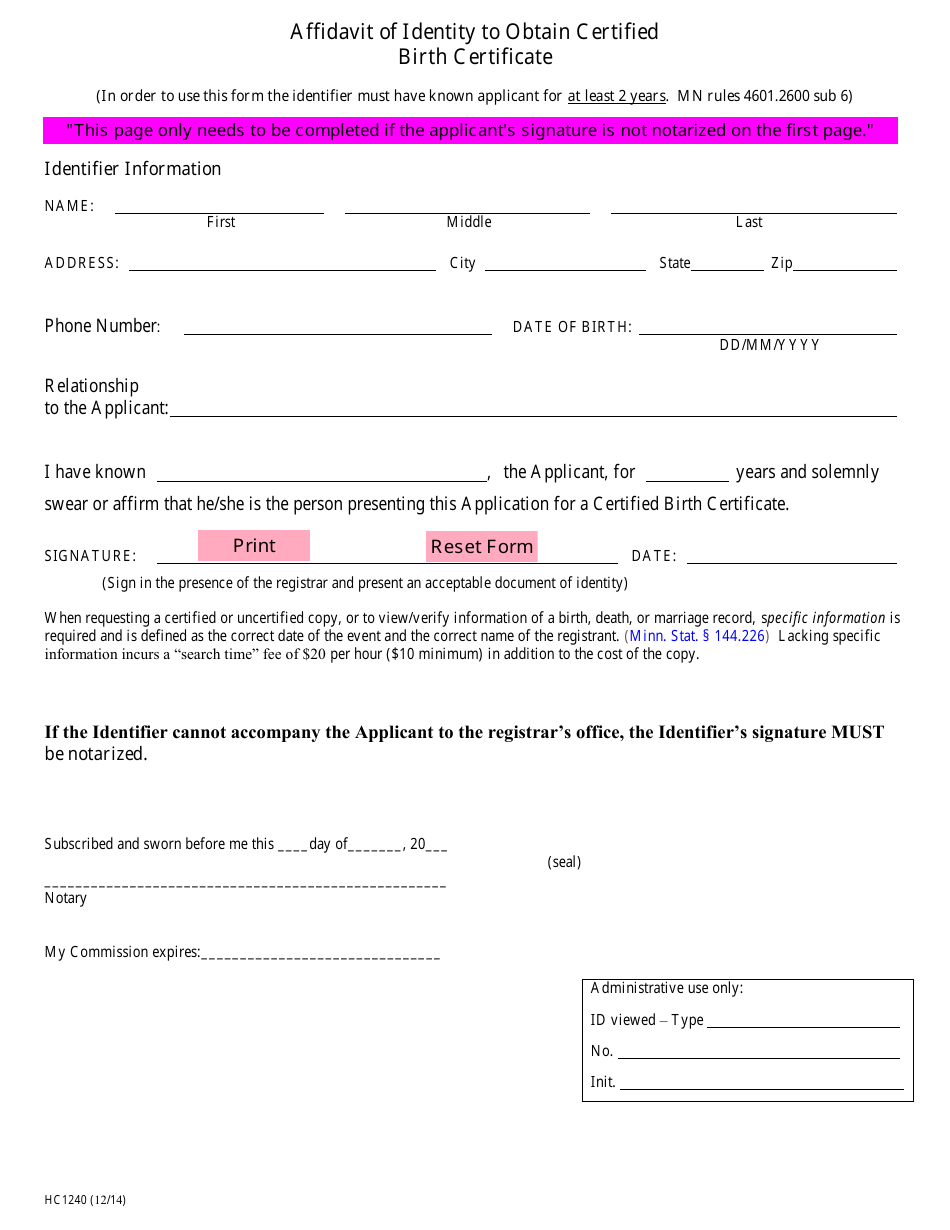
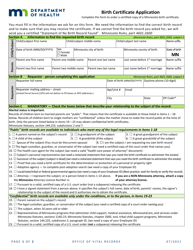
Form HC1240 Birth Certificate Application - County of Hennepin, Minnesota
What Is Form HC1240?
This is a legal form that was released by the County Government - Hennepin County, Minnesota - a government authority operating within Minnesota. The form may be used strictly within County of Hennepin. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
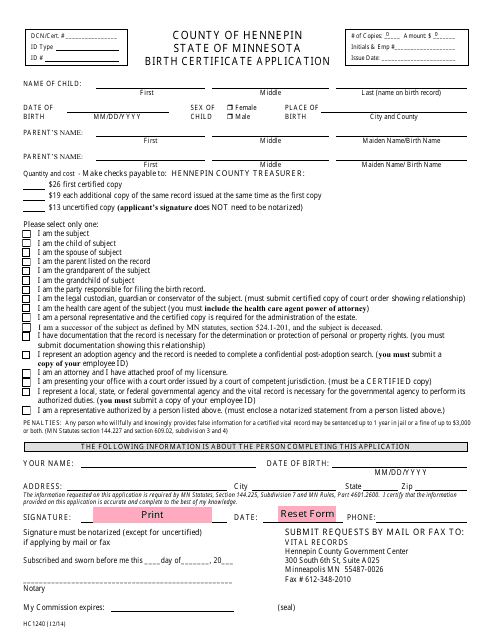
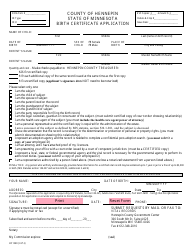
Q: What is Form HC1240?
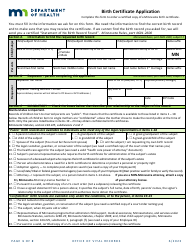
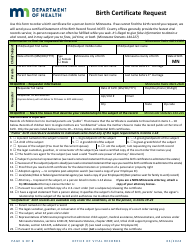
A: Form HC1240 is the Birth Certificate Application for the County of Hennepin, Minnesota.
Q: Who needs to fill out Form HC1240?
A: Form HC1240 needs to be filled out by individuals who want to apply for a birth certificate in Hennepin County, Minnesota.
Q: What is the purpose of Form HC1240?
A: The purpose of Form HC1240 is to provide the necessary information to request a birth certificate in Hennepin County, Minnesota.
Q: How long does it take to process Form HC1240?
A: The processing time for Form HC1240 may vary, but it usually takes a few weeks to receive the requested birth certificate.
Q: Can I request a birth certificate for someone else using Form HC1240?
A: Yes, you can request a birth certificate for someone else using Form HC1240, but additional documentation and authorization may be required.
Form Details:
- Released on December 1, 2014;
- The latest edition provided by the County Government - Hennepin County, Minnesota;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form HC1240 by clicking the link below or browse more documents and templates provided by the County Government - Hennepin County, Minnesota.
Download Form HC1240 Birth Certificate Application - County of Hennepin, Minnesota
1
2