Hospital and Ambulatory Surgical Center Fax Report Form - Massachusetts
Hospital and Ambulatory Surgical Center Fax Report Form is a legal document that was released by the Massachusetts Department of Public Health - a government authority operating within Massachusetts.
FAQ
Q: What is the Hospital and Ambulatory Surgical Center Fax Report Form?
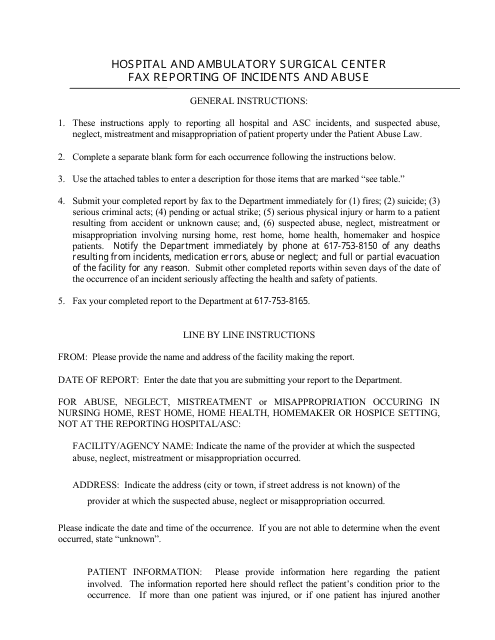
A: The Hospital and Ambulatory Surgical Center Fax Report Form is a document used in Massachusetts to report patient transfers and admissions to hospitals and ambulatory surgical centers.
Q: Who uses the Hospital and Ambulatory Surgical Center Fax Report Form?
A: Healthcare providers and facilities in Massachusetts use the form to communicate patient information and facilitate transfers and admissions.
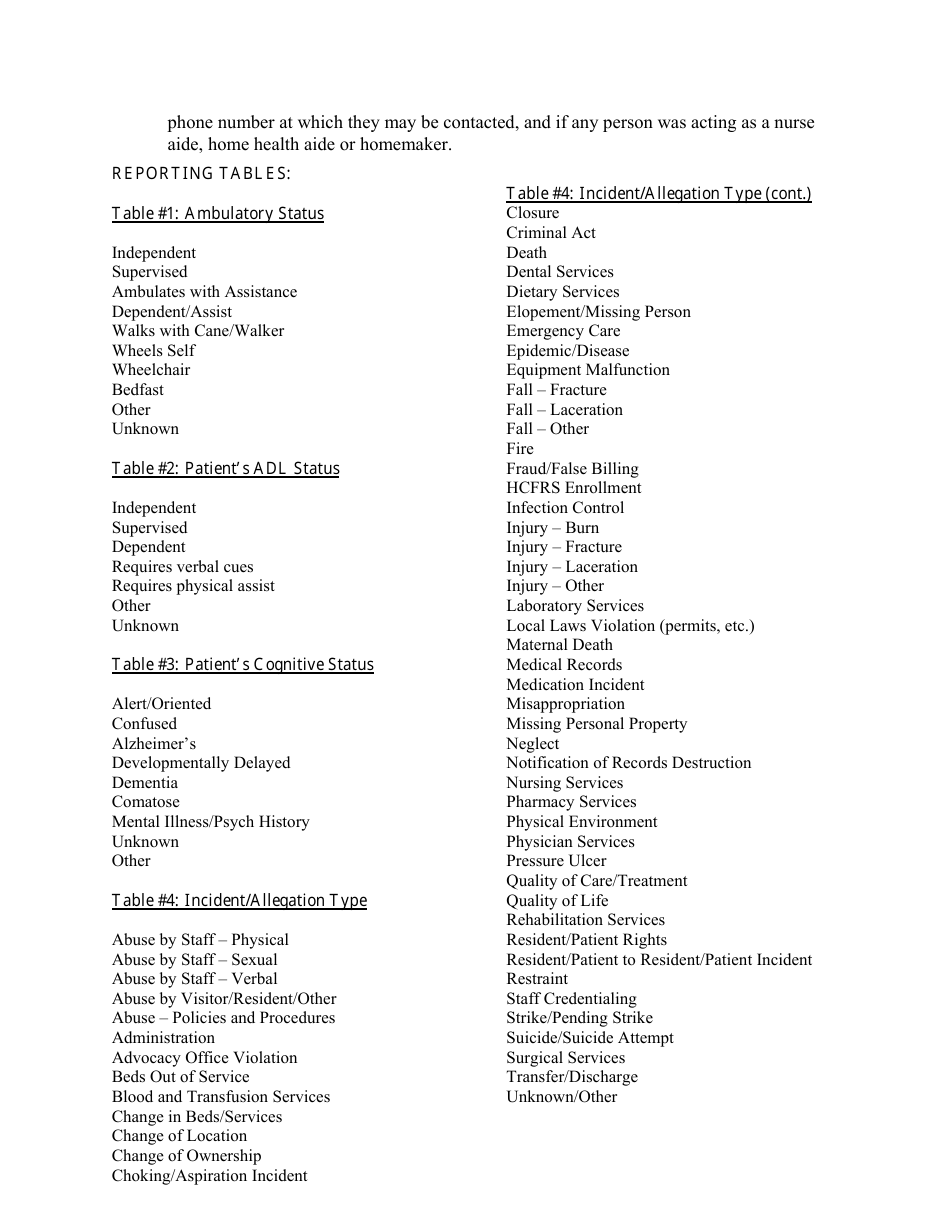
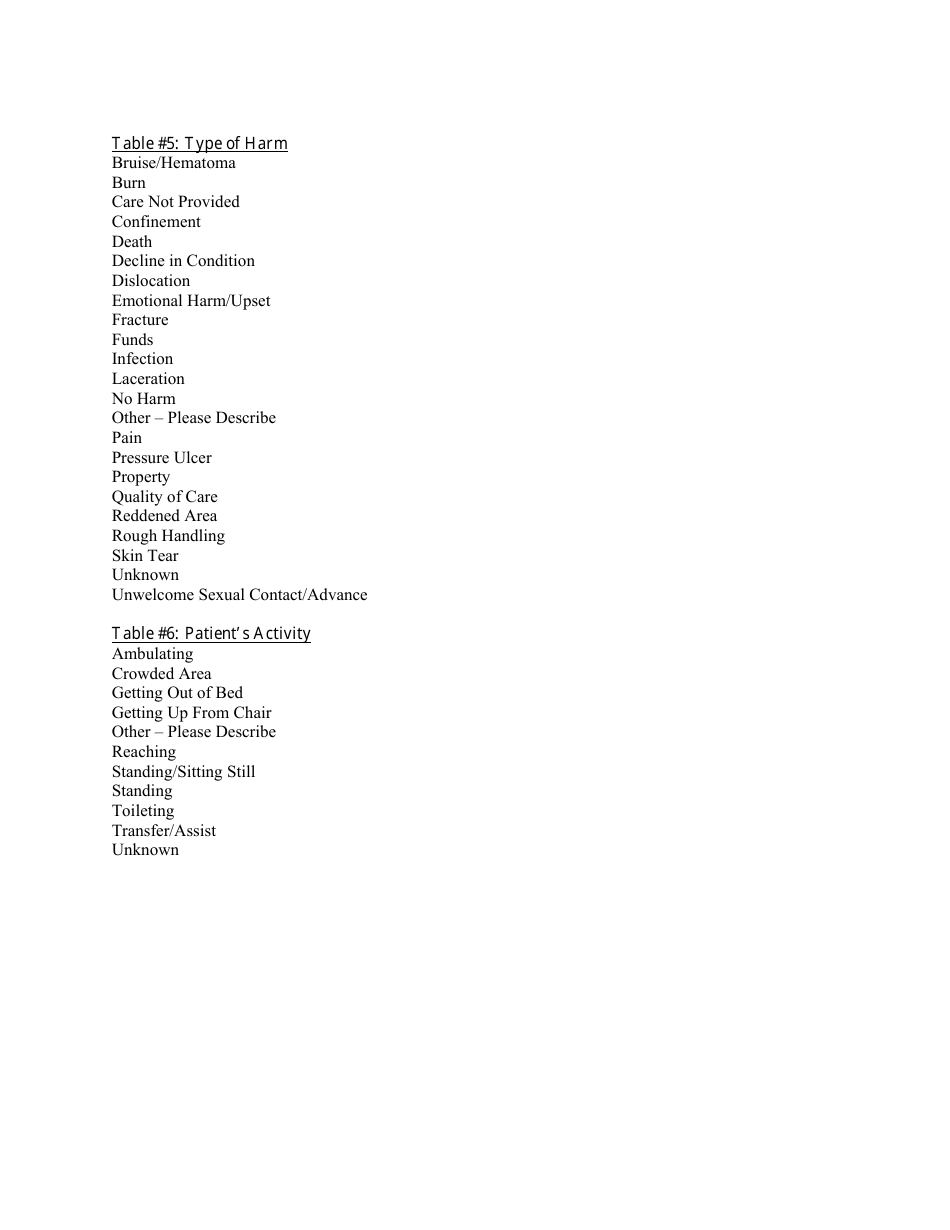
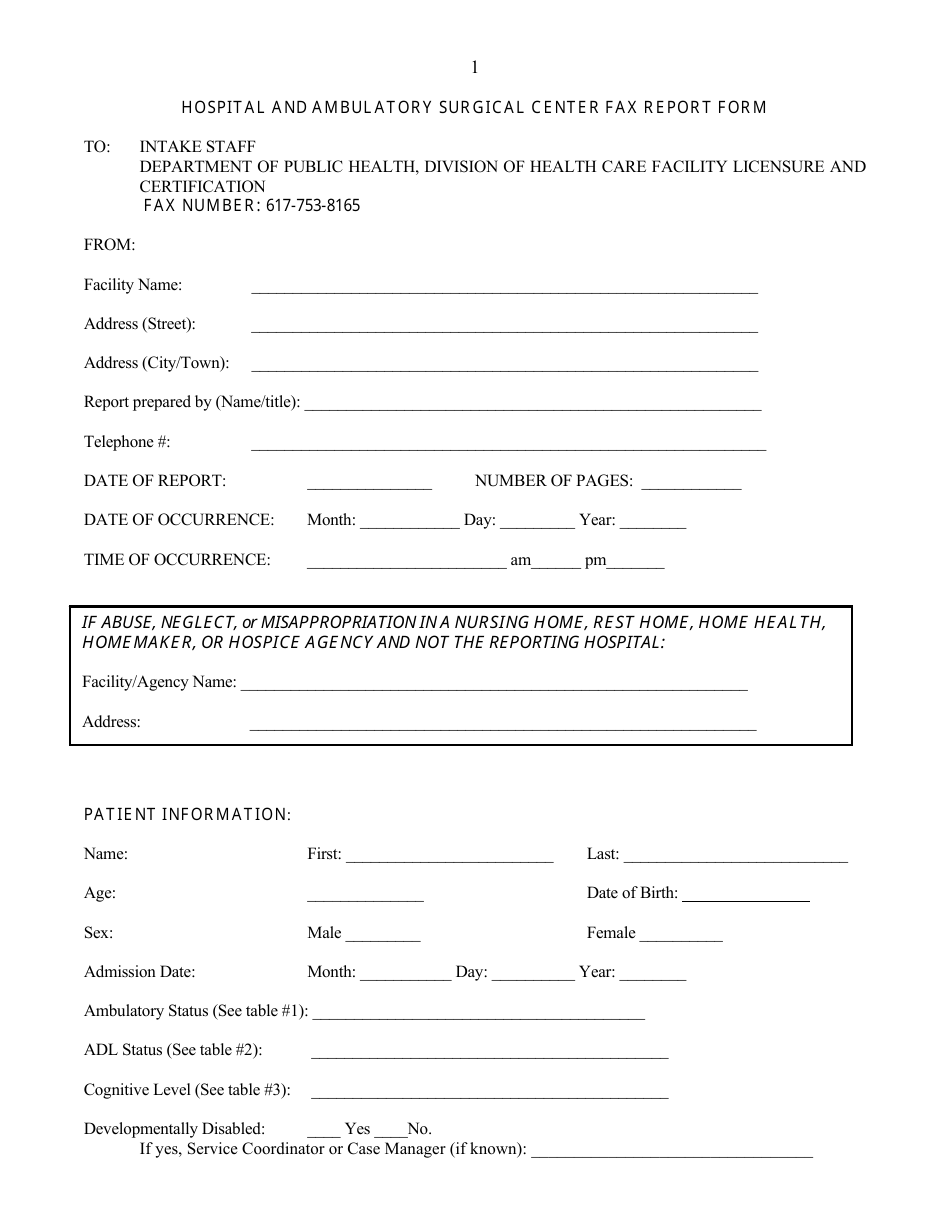
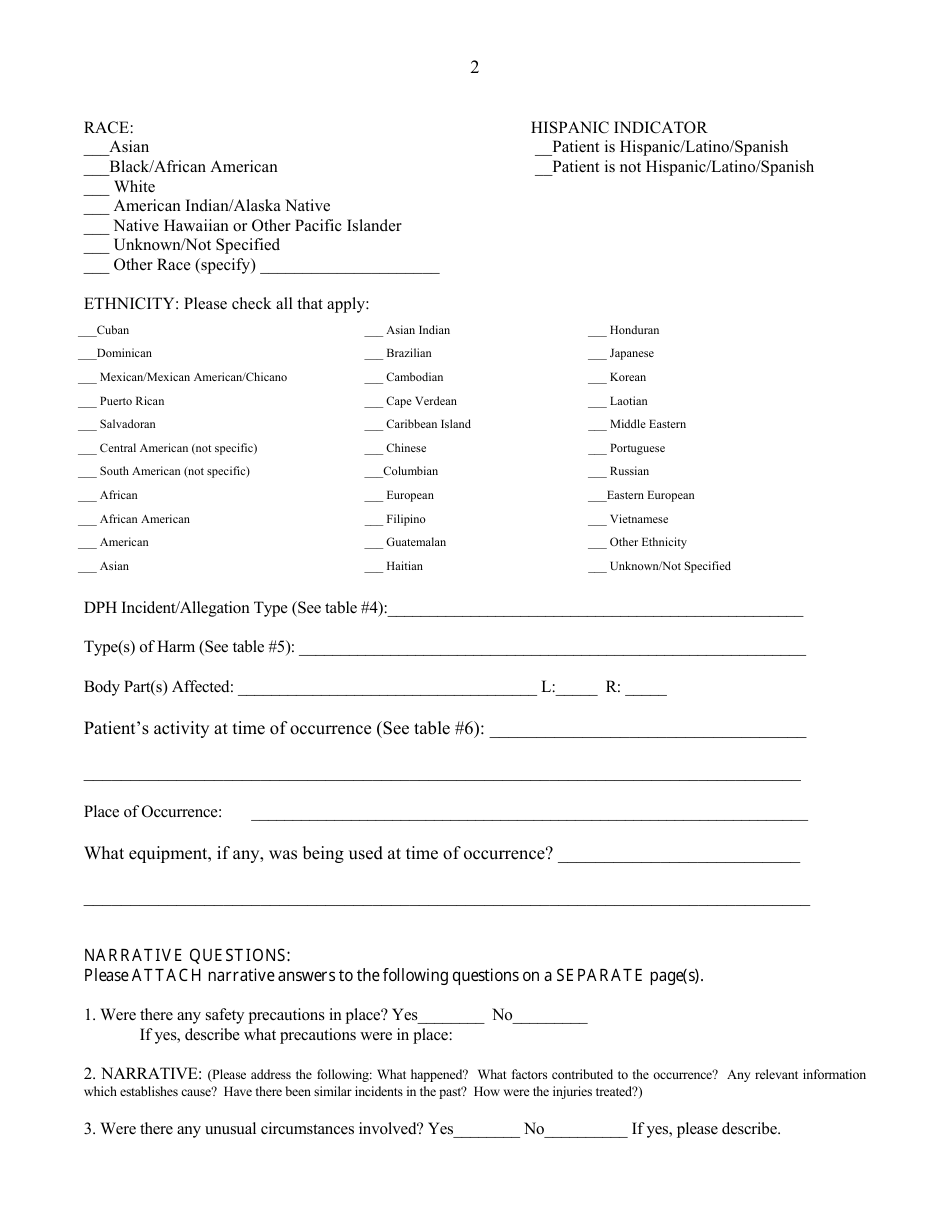
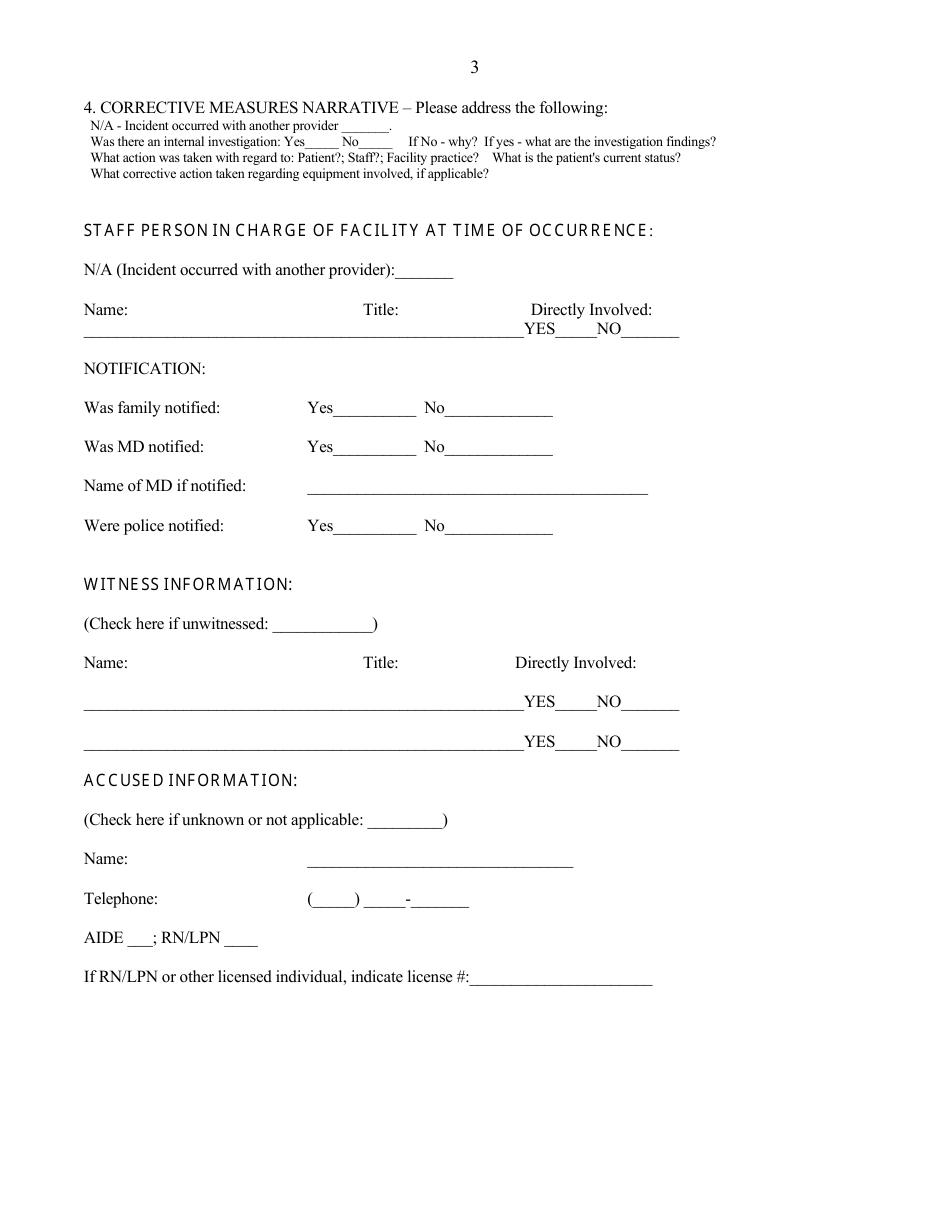
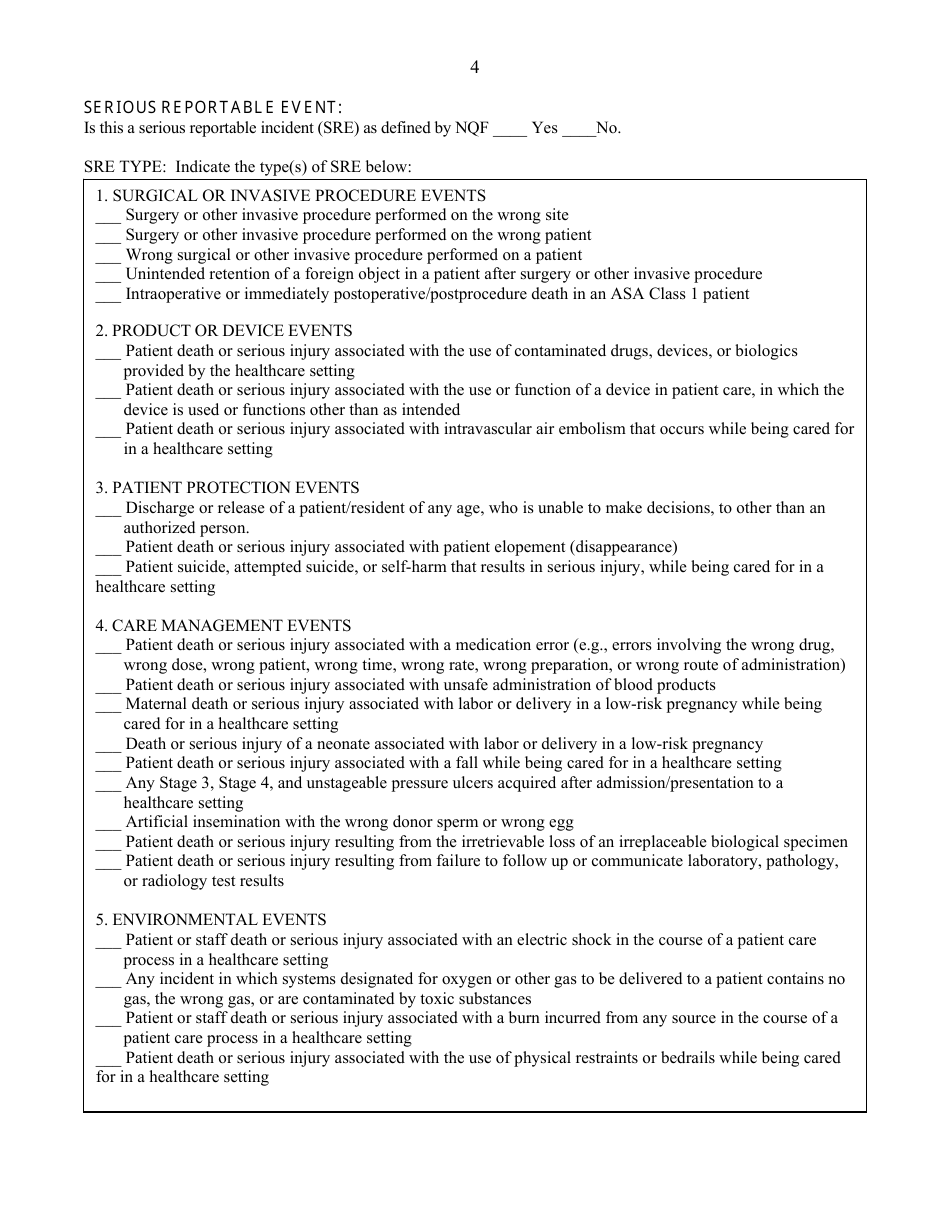
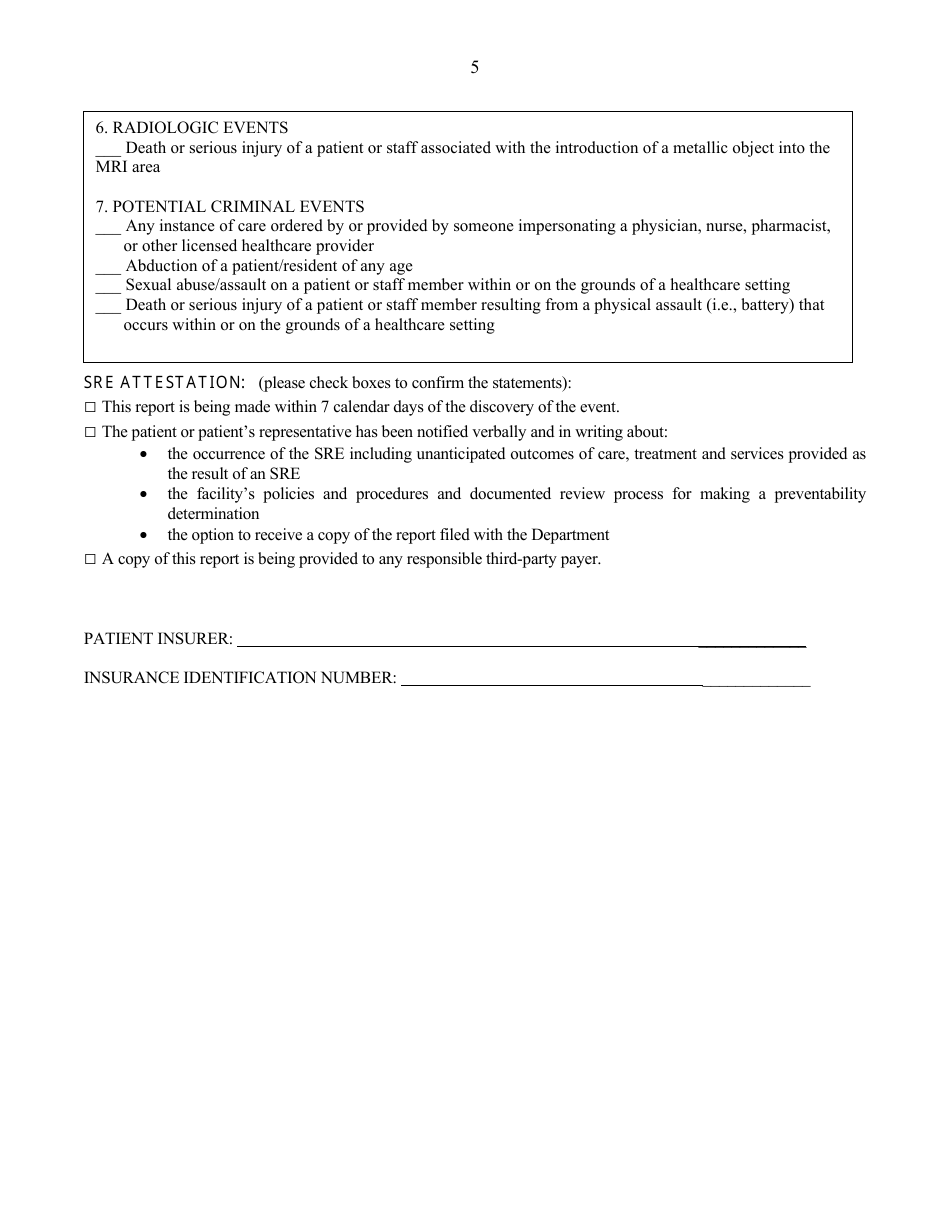
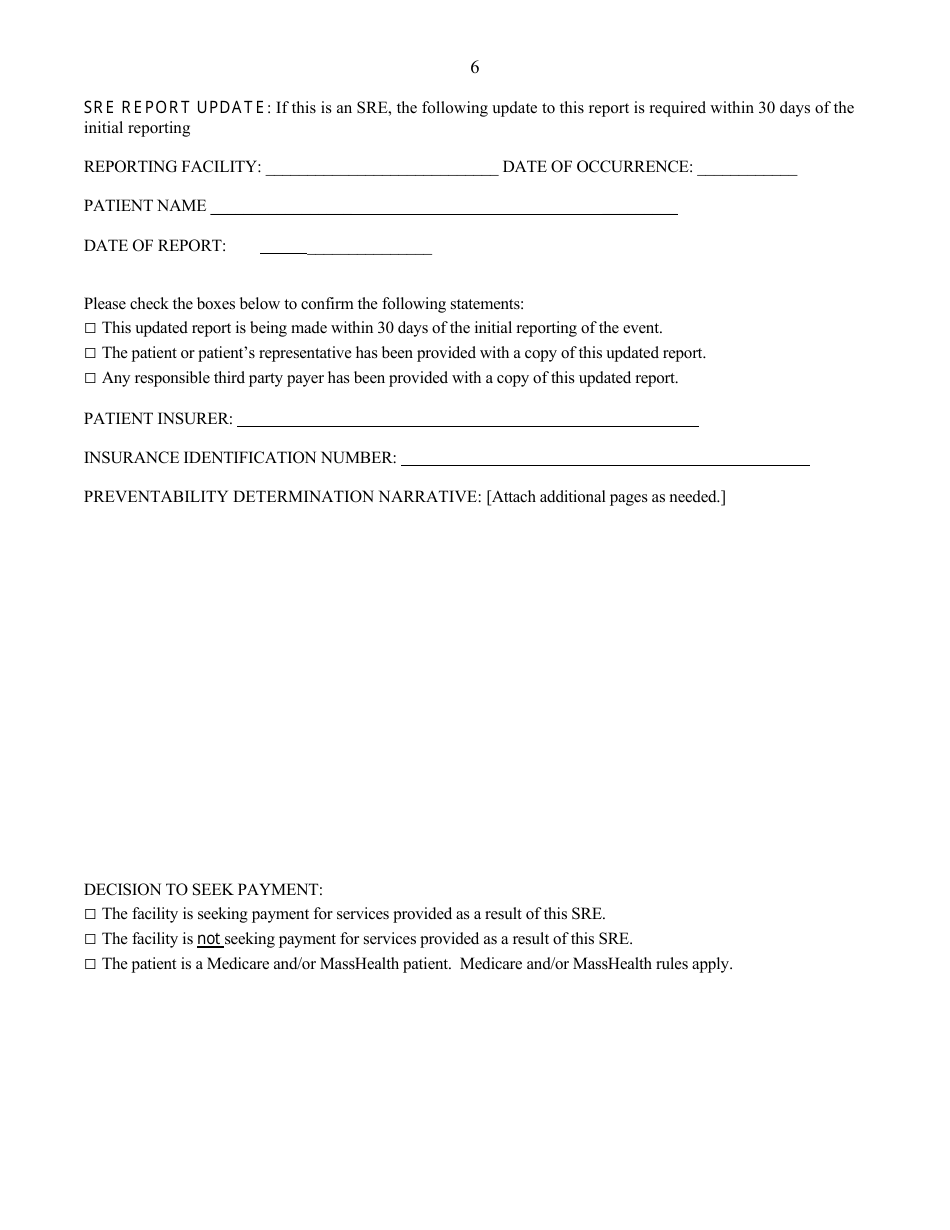
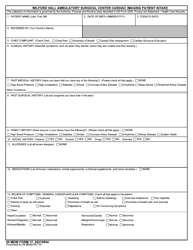
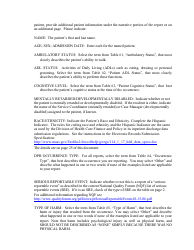
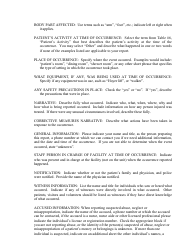
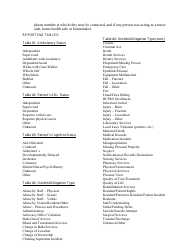
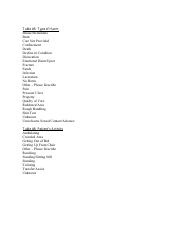
Q: What information is included in the Hospital and Ambulatory Surgical Center Fax Report Form?
A: The form includes information about the patient, referring facility, receiving facility, diagnosis, and emergency contact details, among other relevant details.
Q: Why is the Hospital and Ambulatory Surgical Center Fax Report Form important?
A: The form ensures that necessary information is shared between healthcare providers and facilities during patient transfers and admissions, promoting continuity of care and patient safety.
Form Details:
- The latest edition currently provided by the Massachusetts Department of Public Health;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Massachusetts Department of Public Health.
Download Hospital and Ambulatory Surgical Center Fax Report Form - Massachusetts

1
2
3
4
5
6

7
8
9

10

11