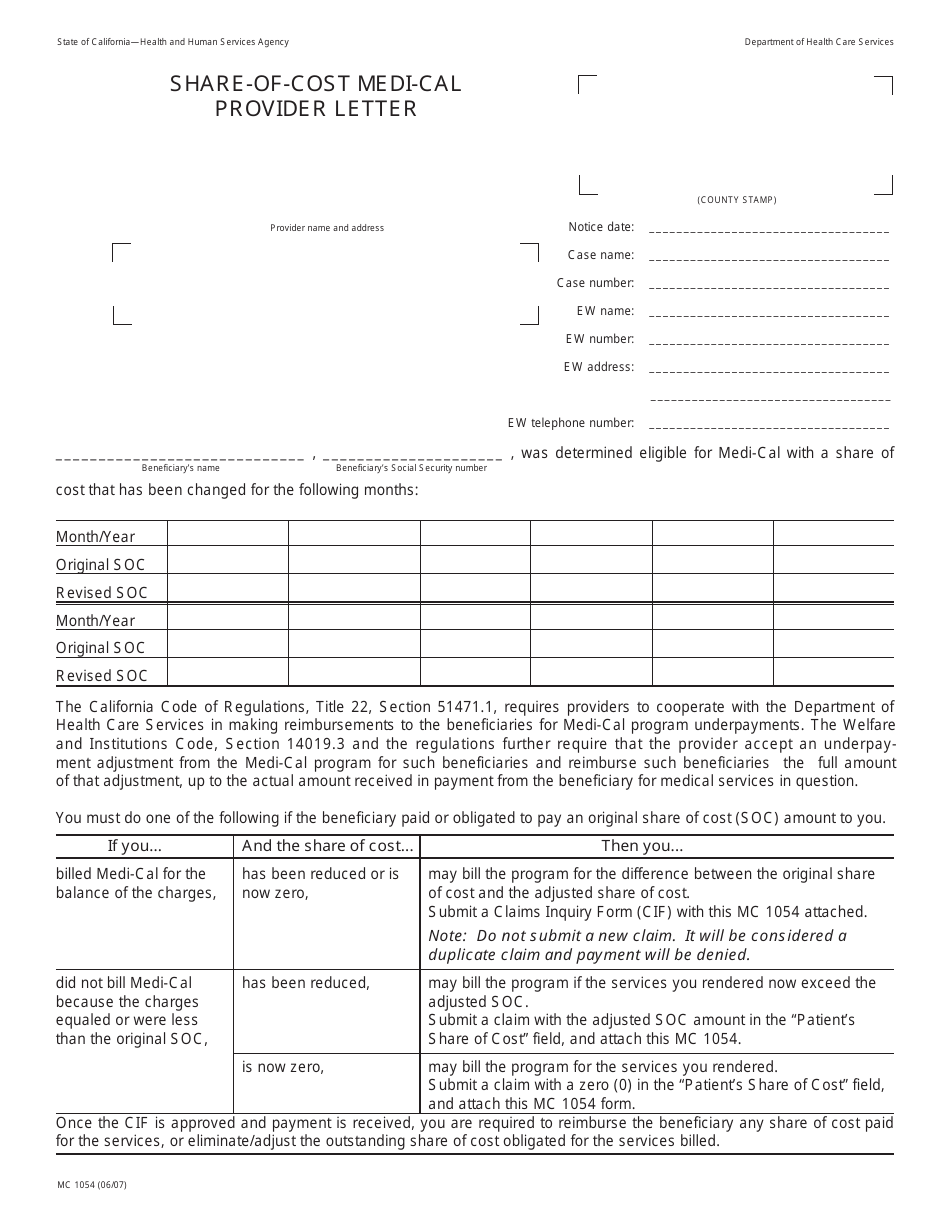
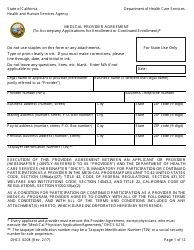
Form MC1054 Share-Of-Cost Medi-Cal Provider Letter - California
What Is Form MC1054?
This is a legal form that was released by the California Department of Health Care Services - a government authority operating within California. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
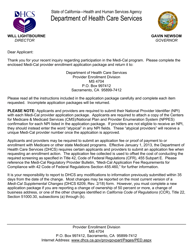
Q: What is the Share-Of-Cost program in Medi-Cal?
A: The Share-Of-Cost program is a way for individuals with higher incomes to qualify for Medi-Cal by paying a certain amount towards their medical expenses each month.
Q: Who is eligible for the Share-Of-Cost program?
A: Individuals who have a higher income but still meet the income and other eligibility requirements for Medi-Cal can qualify for the Share-Of-Cost program.
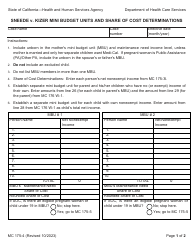
Q: How does the Share-Of-Cost program work?
A: Under the Share-Of-Cost program, individuals are required to pay a certain amount each month before Medi-Cal coverage starts. This amount is based on their income and other factors.
Q: What expenses count towards the Share-Of-Cost?
A: Expenses that are eligible for the Share-Of-Cost include medical bills, prescription drugs, and other healthcare-related costs.
Q: How can providers participate in the Share-Of-Cost program?
A: Providers can participate in the Share-Of-Cost program by accepting patients who have Share-Of-Cost coverage and submitting claims to Medi-Cal for reimbursement.
Form Details:
- Released on June 1, 2007;
- The latest edition provided by the California Department of Health Care Services;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of Form MC1054 by clicking the link below or browse more documents and templates provided by the California Department of Health Care Services.