![]() This version of the form is not currently in use and is provided for reference only. Download this version of
Form CDPH8737
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
Form CDPH8737
for the current year.
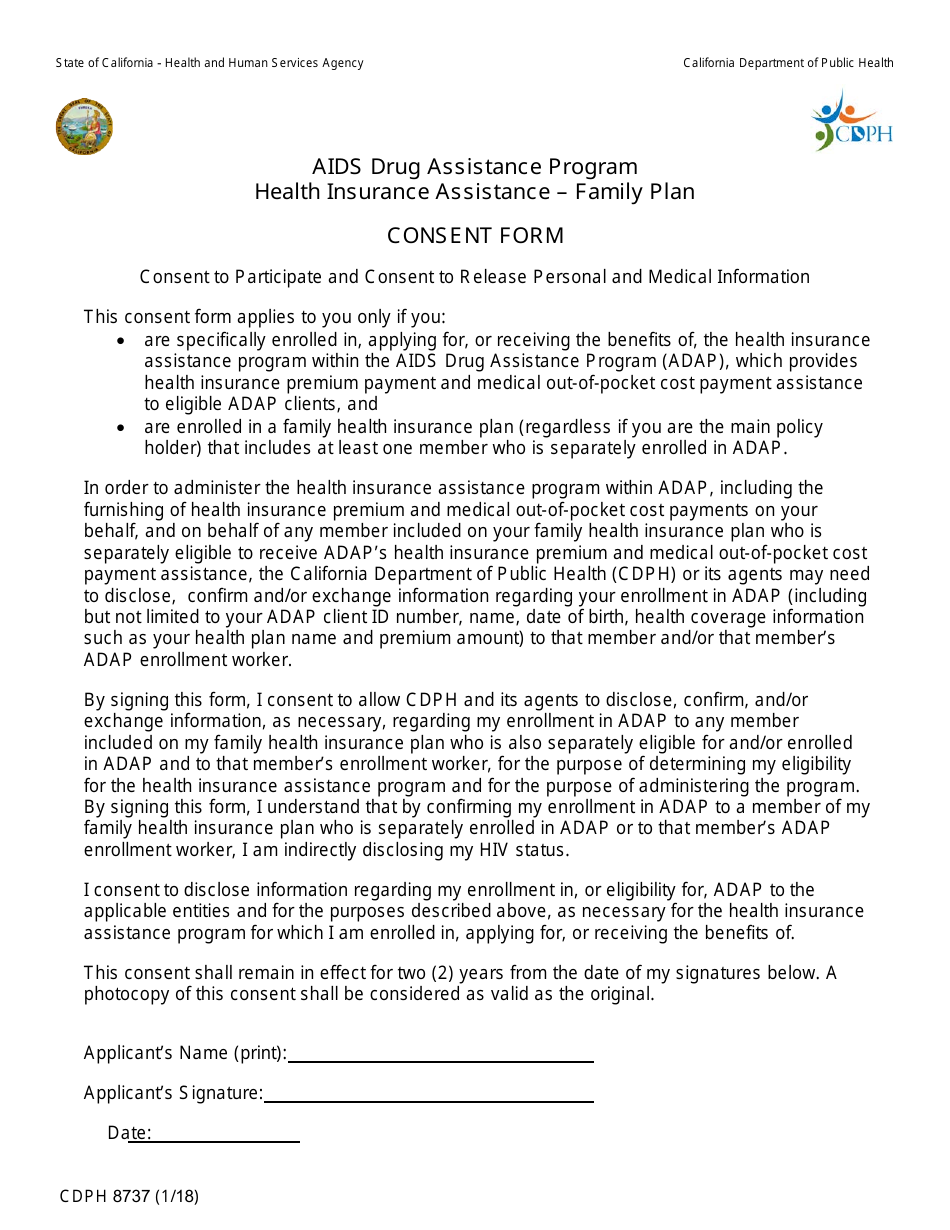
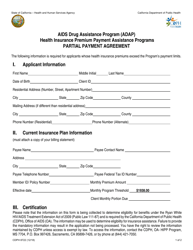
Form CDPH8737 Consent Form - AIDS Drug Assistance Program - Health Insurance Assistance - Family Plan - California
What Is Form CDPH8737?
This is a legal form that was released by the California Department of Public Health - a government authority operating within California. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
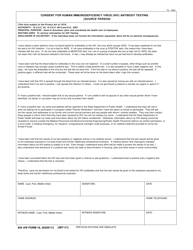
Q: What is the CDPH8737 consent form?
A: The CDPH8737 consent form is a document used for the AIDS Drug Assistance Program, Health Insurance Assistance, and Family Plan in California.
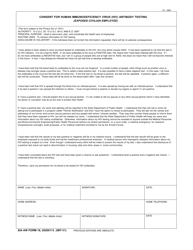
Q: What does the CDPH8737 consent form cover?
A: The CDPH8737 consent form covers various programs including the AIDS Drug Assistance Program, Health Insurance Assistance, and Family Plan in California.
Q: Who needs to fill out the CDPH8737 consent form?
A: Individuals who are applying for the AIDS Drug Assistance Program, Health Insurance Assistance, or Family Plan in California need to fill out the CDPH8737 consent form.
Q: What is the purpose of the CDPH8737 consent form?
A: The purpose of the CDPH8737 consent form is to obtain consent from individuals applying for the AIDS Drug Assistance Program, Health Insurance Assistance, or Family Plan in California.
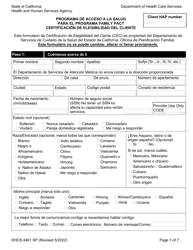
Form Details:
- Released on January 1, 2018;
- The latest edition provided by the California Department of Public Health;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form CDPH8737 by clicking the link below or browse more documents and templates provided by the California Department of Public Health.