Instructions for Form DHCS100187 Drug Medi-Cal (Dmc) Claim Submission Certification - County Operated Provider(S) - California
This document contains official instructions for Form DHCS100187 , Drug Medi-Cal (Dmc) Claim Submission Certification - County Operated Provider(S) - a form released and collected by the California Department of Health Care Services. An up-to-date fillable Form DHCS100187 is available for download through this link.
FAQ
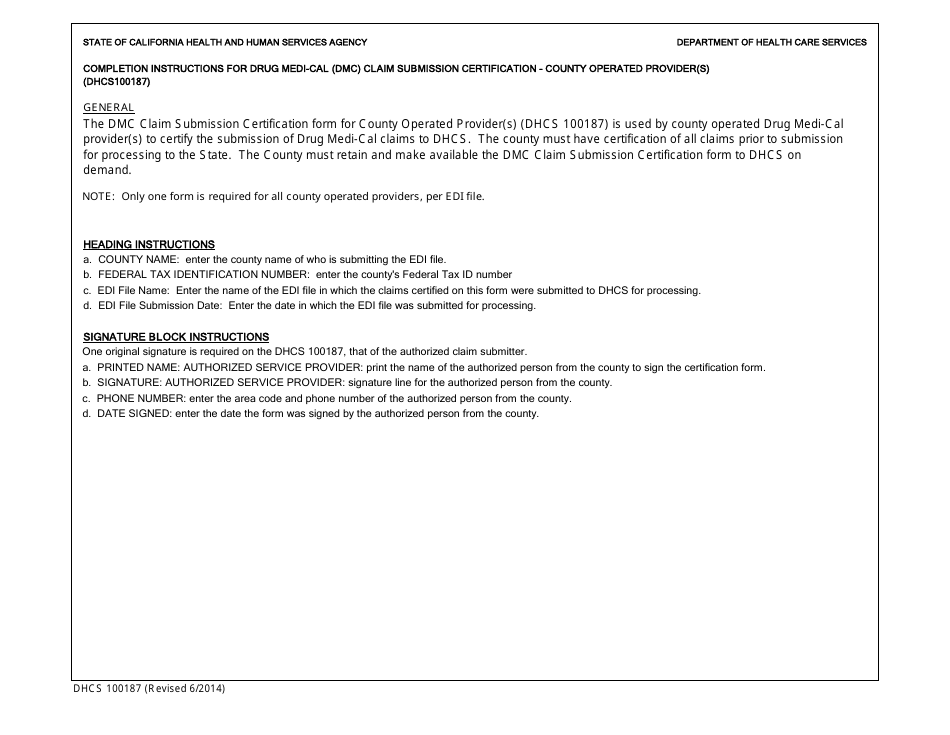
Q: What is Form DHCS100187?
A: Form DHCS100187 is the Drug Medi-Cal (DMC) Claim Submission Certification form for County Operated Providers in California.
Q: Who needs to use this form?
A: This form is specifically for County Operated Providers in California who are submitting claims for the Drug Medi-Cal (DMC) program.
Q: What is the purpose of this form?
A: The purpose of Form DHCS100187 is to certify that the County Operated Provider is in compliance with all requirements for submitting DMC claims.
Q: What information is required on this form?
A: The form requires information such as the provider's name, address, contact information, and certification details.
Q: Are there any additional documents needed with this form?
A: Yes, the form may require additional supporting documents such as copies of provider agreements, licenses, and certifications.
Q: How should the completed form be submitted?
A: The completed form should be submitted electronically to the designated DHCS mailbox or through the DHCS secure file transfer system.
Q: Is there a deadline for submitting this form?
A: Yes, providers must submit the completed form within 15 working days of any changes in the provider's information or certification status.
Q: What happens after the form is submitted?
A: After the form is submitted, DHCS will review the information provided and notify the County Operated Provider of their certification status.
Q: Is there a fee associated with this form?
A: No, there is no fee required for submitting Form DHCS100187.
Instruction Details:
- This 1-page document is available for download in PDF;
- Actual and applicable for the current year;
- Complete, printable, and free.
Download your copy of the instructions by clicking the link below or browse hundreds of other forms in our library of forms released by the California Department of Health Care Services.