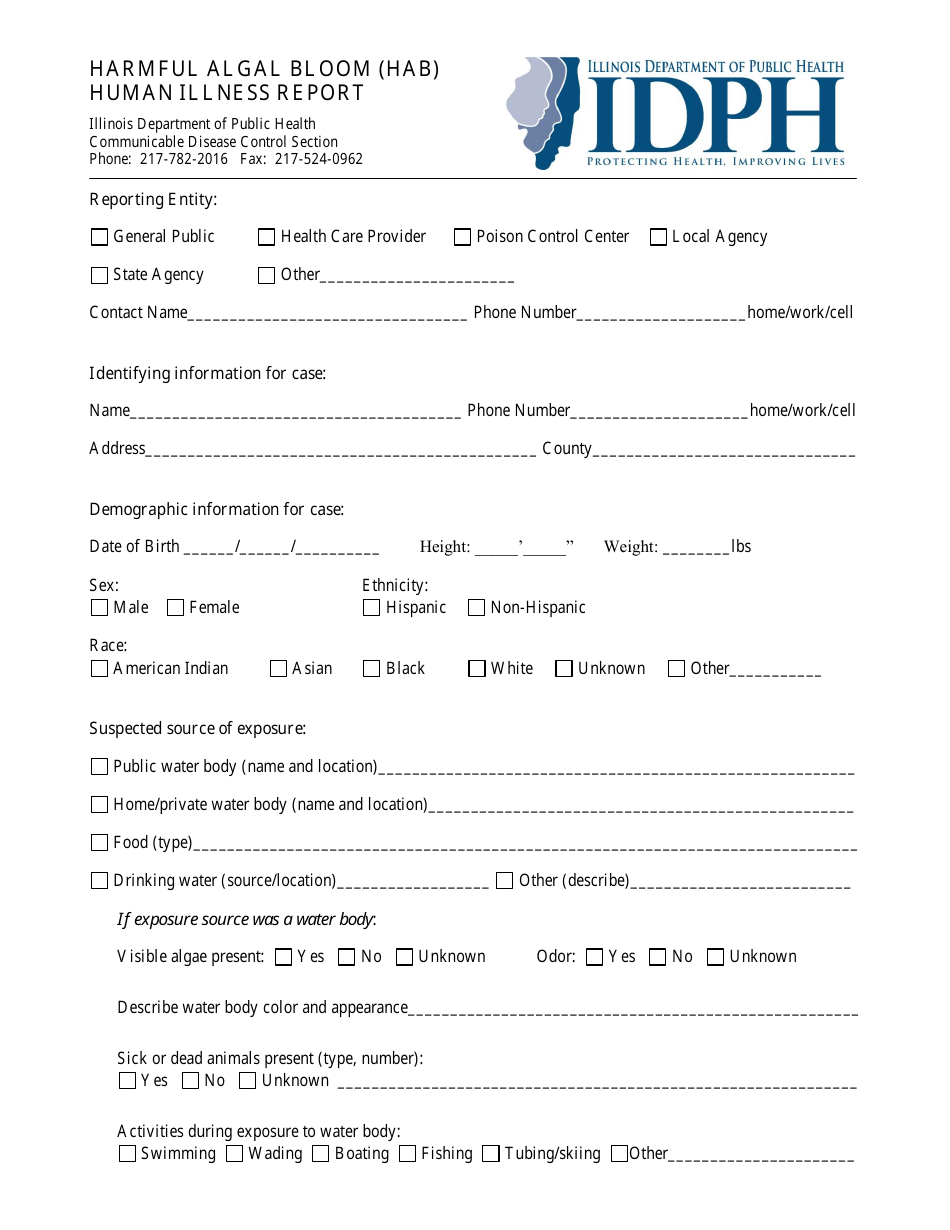
Harmful Algal Bloom (Hab) Human Illness Report Form - Illinois
Harmful Algal Bloom (Hab) Human Illness Report Form is a legal document that was released by the Illinois Department of Public Health - a government authority operating within Illinois.
FAQ
Q: What is Harmful Algal Bloom (HAB)?
A: Harmful Algal Bloom (HAB) is a rapid growth of algae in freshwater or marine environments.
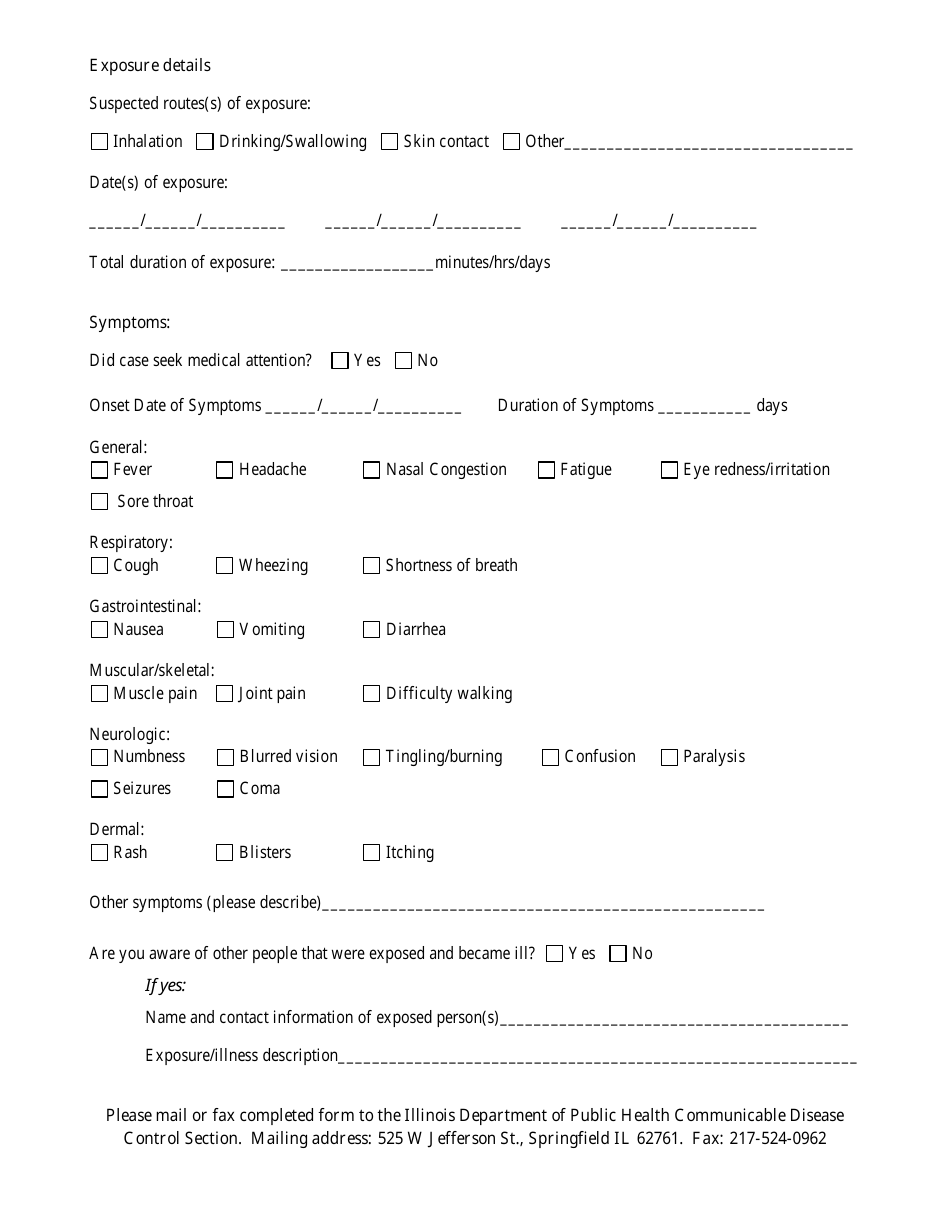
Q: What are the symptoms of HAB-related illnesses?
A: Symptoms of HAB-related illnesses may include skin rashes, respiratory issues, gastrointestinal problems, and neurological effects.
Q: What should I do if I suspect a HAB-related illness?
A: If you suspect a HAB-related illness, you should contact your healthcare provider and report the illness to the appropriate authorities.
Q: How can I report a HAB-related illness in Illinois?
A: In Illinois, you can report a HAB-related illness using the Harmful Algal Bloom (HAB) Human Illness Report Form.
Q: Why is it important to report HAB-related illnesses?
A: Reporting HAB-related illnesses helps authorities track and monitor the presence of harmful algal blooms and take appropriate actions to protect public health.
Q: What can I do to prevent HAB-related illnesses?
A: To prevent HAB-related illnesses, avoid contact with water that appears discolored, foamy, or has a strong odor. It is also important to follow any advisories or warnings issued by health or environmental officials.
Q: Are HAB-related illnesses contagious?
A: No, HAB-related illnesses are not contagious. They are caused by exposure to toxins produced by harmful algal blooms.
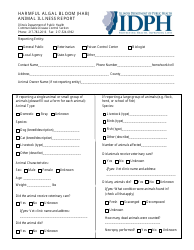
Q: Can pets be affected by HAB-related illnesses?
A: Yes, pets can be affected by HAB-related illnesses. It is important to keep them away from water sources experiencing harmful algal blooms.
Form Details:
- The latest edition currently provided by the Illinois Department of Public Health;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Illinois Department of Public Health.
Download Harmful Algal Bloom (Hab) Human Illness Report Form - Illinois

1

2