Form DOH-5199 Member Request for Specific Protected Medicaid Health Information - New York
What Is Form DOH-5199?
This is a legal form that was released by the New York State Department of Health - a government authority operating within New York. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is the Form DOH-5199?
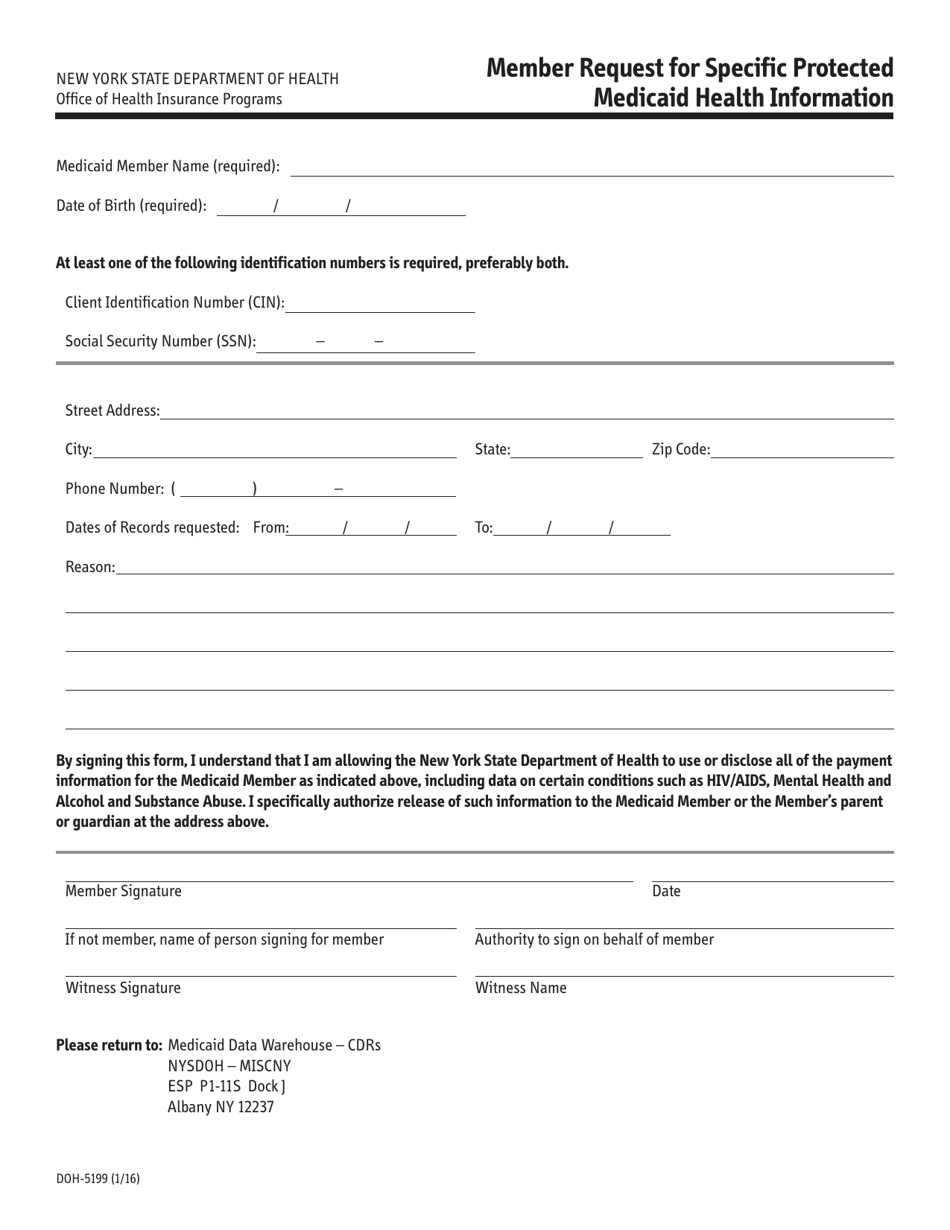
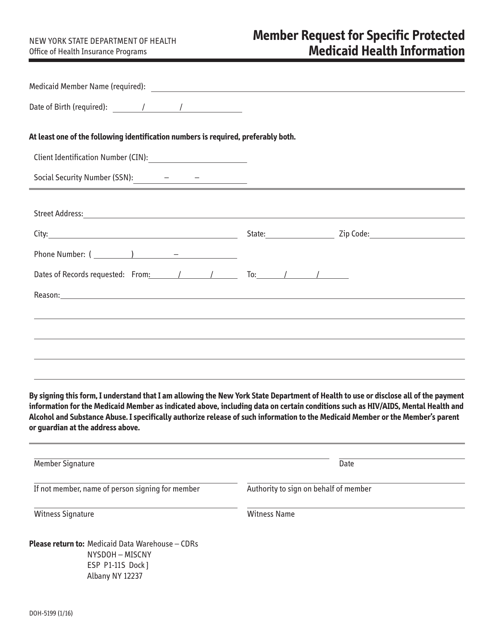
A: Form DOH-5199 is a Member Request for Specific Protected Medicaid Health Information in New York.
Q: Who can use the Form DOH-5199?
A: This form can be used by individuals who are enrolled in Medicaid and want to request specific protected health information.
Q: What is the purpose of Form DOH-5199?
A: The purpose of this form is to allow Medicaid enrollees to request access to their own protected health information.
Q: What information is required on Form DOH-5199?
A: The form requires you to provide personal information, such as your name, Medicaid ID, and the specific health information you are requesting.
Q: Can I authorize someone else to request my health information?
A: Yes, you can authorize another person to request your health information by completing the "Authorization to Act as Member's Representative" section of the form.
Q: How long does it take to process a request made with Form DOH-5199?
A: The processing time for requests made with Form DOH-5199 may vary, but generally, you should allow for at least 30 days.
Q: Is there a fee for requesting health information using Form DOH-5199?
A: There is no fee for requesting health information using Form DOH-5199.
Q: Can I request information about someone else using this form?
A: No, Form DOH-5199 is specifically for requesting your own protected health information. If you need to request information about someone else, you may need to use a different form or process.
Q: What should I do if my request is denied?
A: If your request is denied, you have the right to appeal the decision. The denial notice should provide information on how tofile an appeal.
Form Details:
- Released on January 1, 2016;
- The latest edition provided by the New York State Department of Health;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of Form DOH-5199 by clicking the link below or browse more documents and templates provided by the New York State Department of Health.