Instructions for Adult Day Intake Screening - Pennsylvania
This document was released by Pennsylvania Department of Aging and contains the most recent official instructions for Adult Day Intake Screening .
FAQ
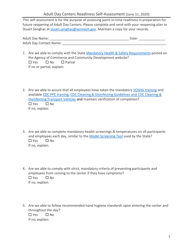
Q: What is an Adult Day Intake Screening?
A: An Adult Day Intake Screening is an assessment process to determine the eligibility and appropriateness of an individual for an adult day program in Pennsylvania.
Q: Who conducts the Adult Day Intake Screening?
A: The Adult Day Intake Screening is conducted by a qualified professional, such as a social worker or nurse.
Q: What is the purpose of the Adult Day Intake Screening?
A: The purpose of the Adult Day Intake Screening is to evaluate an individual's physical, cognitive, and social functioning to ensure they can benefit from and safely participate in an adult day program.
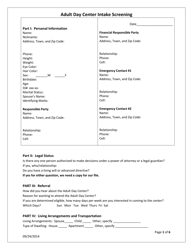
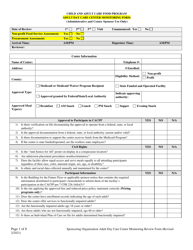
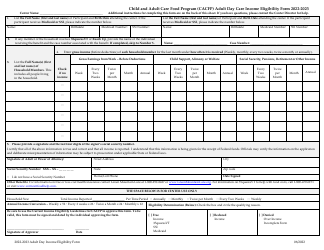
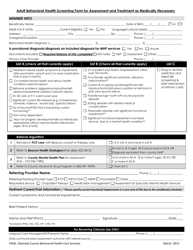
Q: What information is collected during the Adult Day Intake Screening?
A: During the Adult Day Intake Screening, information about the individual's medical history, current medications, functional abilities, and social support network is collected.
Q: How long does the Adult Day Intake Screening take?
A: The duration of the Adult Day Intake Screening may vary, but it typically takes about 1-2 hours.
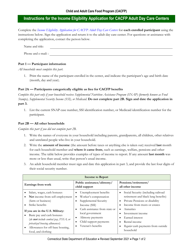
Q: Is there a cost associated with the Adult Day Intake Screening?
A: There may be a cost associated with the Adult Day Intake Screening. It is recommended to check with the specific adult day program for details on any fees or insurance coverage.
Q: What happens after the Adult Day Intake Screening?
A: After the Adult Day Intake Screening, a determination is made regarding the individual's eligibility and appropriateness for the adult day program. If approved, the individual can proceed with enrollment.
Q: Can a family member or caregiver be present during the Adult Day Intake Screening?
A: Yes, a family member or caregiver can be present during the Adult Day Intake Screening to provide additional information and support.
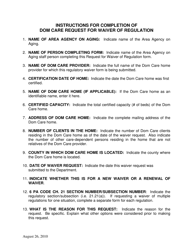
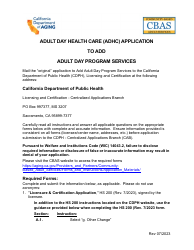
Q: Are there any requirements for participating in an adult day program in Pennsylvania?
A: Each adult day program may have specific requirements for participation, such as age restrictions or medical conditions. It is important to contact the program directly for information on their eligibility criteria.
Instruction Details:
- This 2-page document is available for download in PDF;
- Actual and applicable for the current year;
- Complete, printable, and free.
Download your copy of the instructions by clicking the link below or browse hundreds of other forms in our library legal documents released by the Pennsylvania Department of Aging.
1

2