Form CMS-1500 Health Insurance Claim Form
What Is a Health Insurance Claim Form?
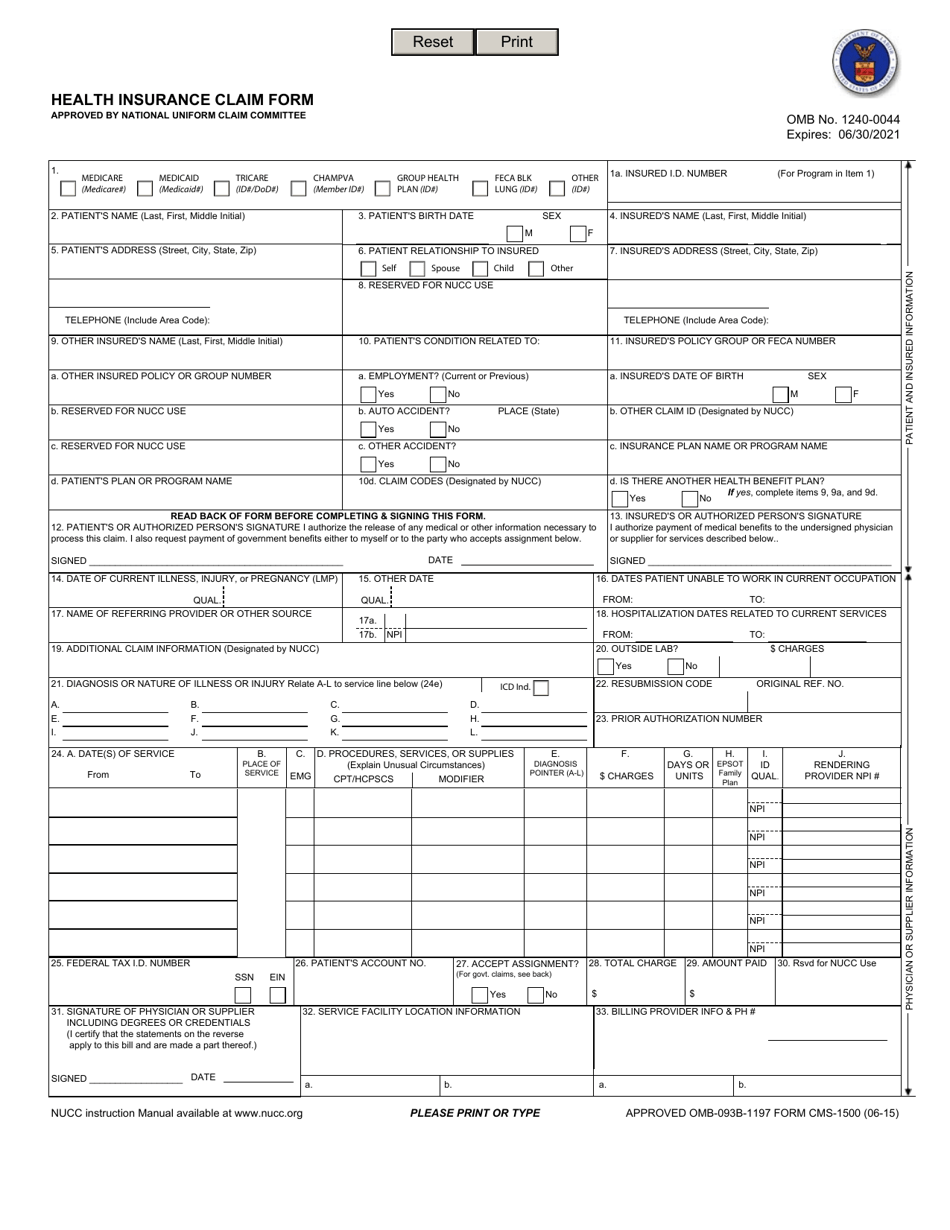
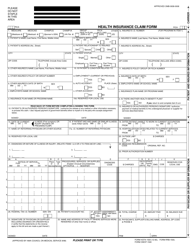
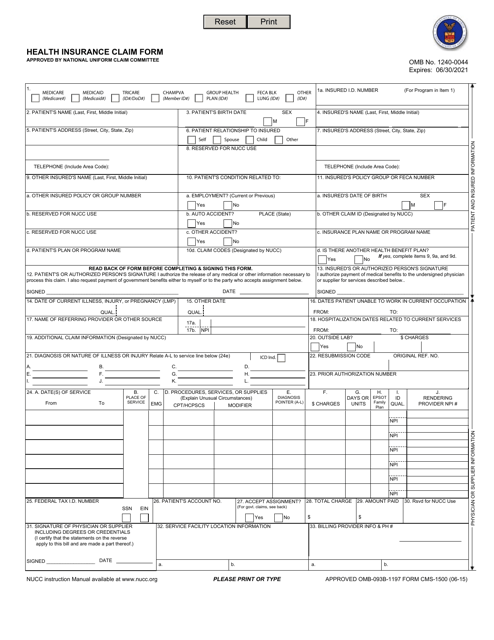
Form CMS-1500, Health Insurance Claim Form , is a legal document used by physicians and other healthcare providers and professionals to submit claims for medical services. It answers the needs of many healthcare payers and is accepted nationwide by most insurance companies as the physician statement for submission of medical claims. Form CMS-1500 provides information about the patient and insured, their diagnosis, treatment, and insurance details.
Former Names:
- Form HCFA-1500;
- Form RRB-1500;
- Form OWCP-1500.
This form was released by the Centers for Medicare & Medicaid Services , a component of the U.S. Department of Health and Human Services , on June 1, 2015 , with all previous editions obsolete. You can download a Health Insurance Claim Form 1500 fillable version through the link below.
How to Fill Out a Health Insurance Claim Form?
-
The first section of the Health Insurance Claim Form CMS-1500 must be completed by the patient and insured:
- State the type of health insurance applicable to this claim and the insured's ID number;
- Write down the patient's full name, birth date, sex, and address. Enter the insured's full name, address, and the patient's relationship to the insured - "self" means the insured is the patient;
- If there is an additional group health coverage, state the other insured's full name, policy or group number, and insurance plan or program name;
- If the patient's condition is related to employment, auto accident or other accident, check the appropriate box;
- Enter the appropriate claim codes issued by the National Uniform Claim Committee;
- Record the insured's policy or group number, date of birth, sex, and insurance plan or program name;
- Sign and date the form. The claim form requires the signatures of the patient and the insured or their authorized representatives.
-
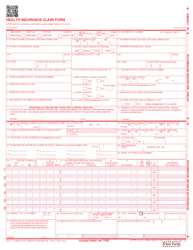
The second section of the CMS-1500 Form is for the physician:
- Enter the date of current illness, injury, or pregnancy;
- Add another date related to the patient's treatment and the period of time the patient is unable to work;
- Name the professional who orders the services on the claim and state their National Provider Identifier number;
- Indicate the hospitalization dates and report additional claim information;
- If the medical services were rendered by an independent provided, record the related costs;
- State the diagnosis or nature of injury or illness;
- If you resubmit the claim, add the original reference number;
- Enter the payer assigned number authorizing the services;
- State the dates and place of services, add the emergency indicator if needed, list the procedures and services provided, and state the reason they were performed. Write down the charge amount for each service and the number of days or units, identify services covered under state plans and the rendering provider;
- Write down the billing provider Federal Tax ID number and patient's account number. Agree to accept assignment under the terms of the payer's program;
- State the total charge and the amount paid;
- Sign and date the form. Enter the location where the services were rendered and the provider's or supplier's billing name and address.
Download Form CMS-1500 Health Insurance Claim Form
1
2
3

4