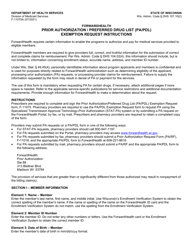
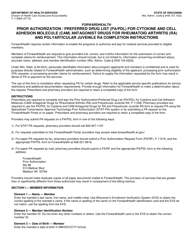
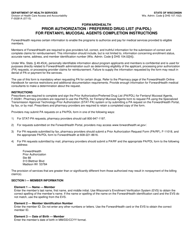
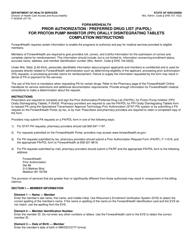
Instructions for Form F-11307 Rior Authorization / Preferred Drug List (Pa / Pdl) for Cytokine and Cell Adhesion Molecule (Cam) Antagonist Drugs for Psoriatic Arthritis - Wisconsin
This document contains official instructions for Form F-11307 , Rior Authorization/Preferred Cell Adhesion Molecule (Cam) Antagonist Drugs for Psoriatic Arthritis - a form released and collected by the Wisconsin Department of Health Services.
FAQ
Q: What is Form F-11307?
A: Form F-11307 is an authorization form for Preferred Drug List (Pa/Pdl) for Cytokine and Cell Adhesion Molecule (Cam) Antagonist Drugs for Psoriatic Arthritis in Wisconsin.
Q: What is Psoriatic Arthritis?
A: Psoriatic Arthritis is a type of arthritis that affects people with psoriasis, causing joint pain, swelling, and stiffness.
Q: Who needs to fill out Form F-11307?
A: This form needs to be filled out by patients or their healthcare providers who are seeking authorization for a specific drug treatment for Psoriatic Arthritis.
Q: What is the purpose of Form F-11307?
A: The purpose of Form F-11307 is to request prior authorization for the use of Cytokine and Cell Adhesion Molecule Antagonist Drugs for the treatment of Psoriatic Arthritis.
Q: What is the Preferred Drug List (Pa/Pdl)?
A: The Preferred Drug List (Pa/Pdl) is a list of medications approved by Wisconsin's Medicaid program for coverage under specific medical conditions, such as Psoriatic Arthritis.
Instruction Details:
- This 3-page document is available for download in PDF;
- Actual and applicable for the current year;
- Complete, printable, and free.
Download your copy of the instructions by clicking the link below or browse hundreds of other forms in our library of forms released by the Wisconsin Department of Health Services.
Download Instructions for Form F-11307 Rior Authorization / Preferred Drug List (Pa / Pdl) for Cytokine and Cell Adhesion Molecule (Cam) Antagonist Drugs for Psoriatic Arthritis - Wisconsin
1
2

3