Form SFN54044 Authorization for Disclosure of Protected Health Information - North Dakota
What Is Form SFN54044?
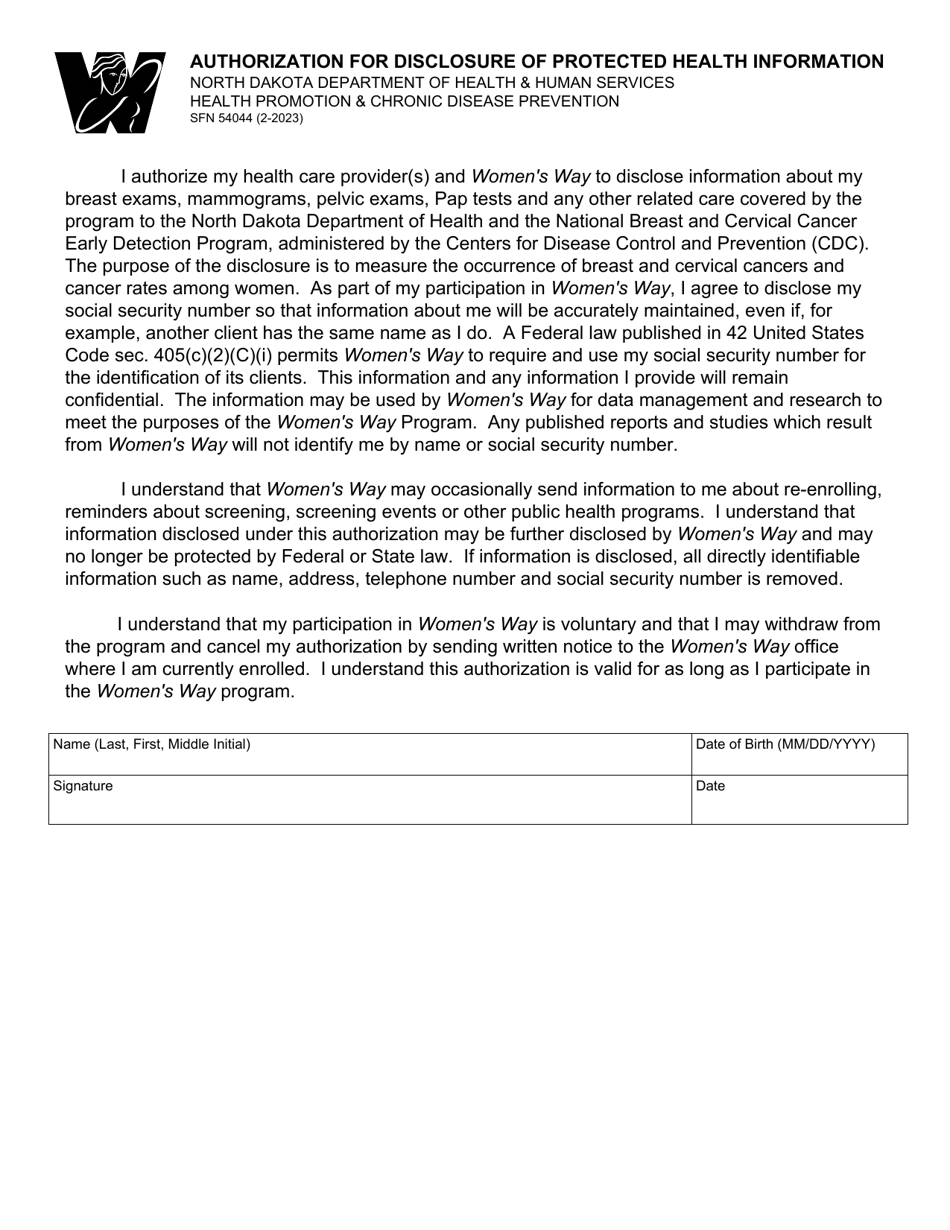
This is a legal form that was released by the North Dakota Department of Health and Human Services - a government authority operating within North Dakota. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is Form SFN54404?
A: Form SFN54404 is the Authorization for Disclosure of Protected Health Information specific to North Dakota.
Q: Why do I need to fill out Form SFN54404?
A: You need to fill out Form SFN54404 to authorize the disclosure of your protected health information in North Dakota.
Q: What information do I need to provide on Form SFN54404?
A: You will need to provide your personal information, the information of the person or entity authorized to receive your health information, and the purpose for which the information will be disclosed.
Q: Are there any fees associated with submitting Form SFN54404?
A: There may be fees associated with submitting Form SFN54404. You should contact the North Dakota Department of Health for more information.
Form Details:
- Released on February 1, 2023;
- The latest edition provided by the North Dakota Department of Health and Human Services;
- Easy to use and ready to print;
- Available in Spanish;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form SFN54044 by clicking the link below or browse more documents and templates provided by the North Dakota Department of Health and Human Services.