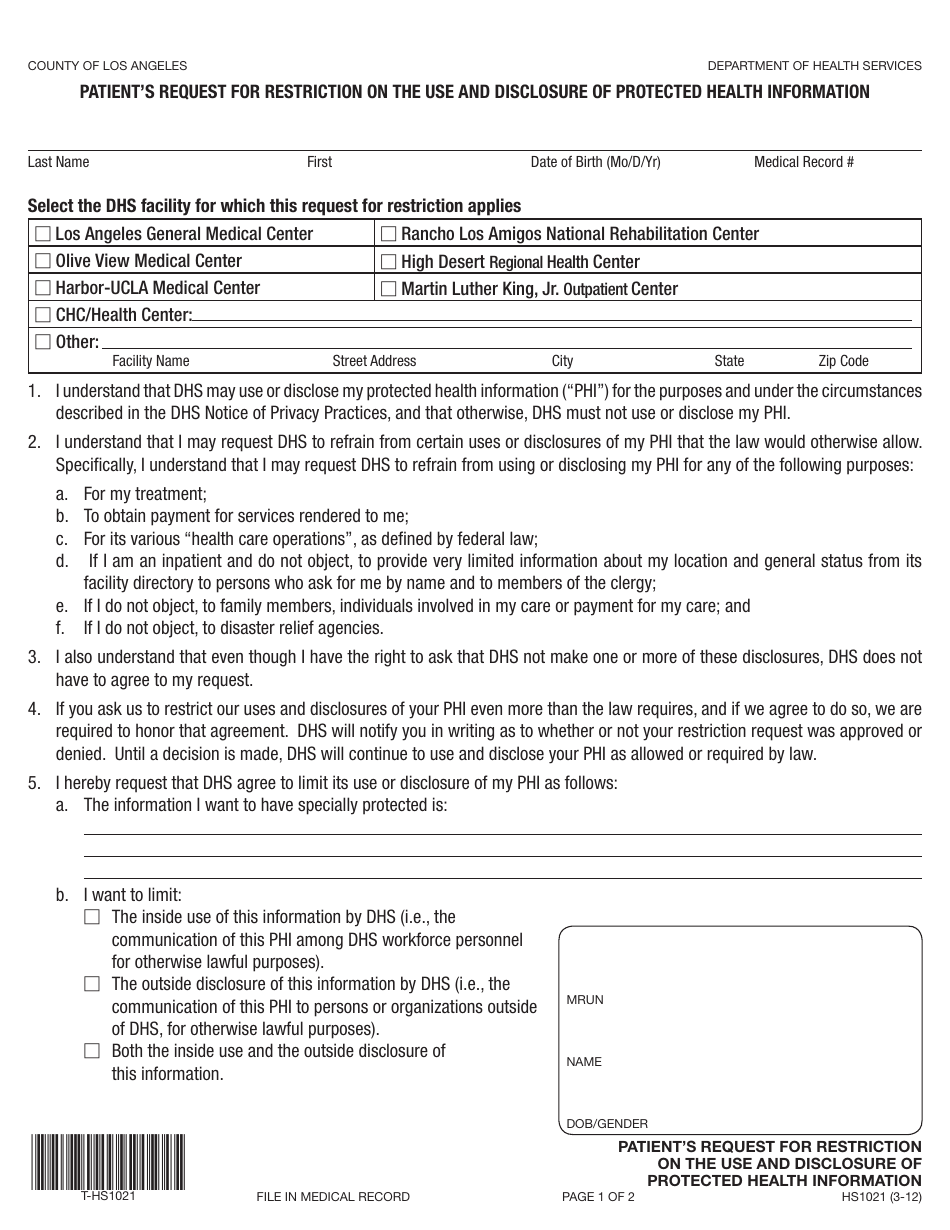
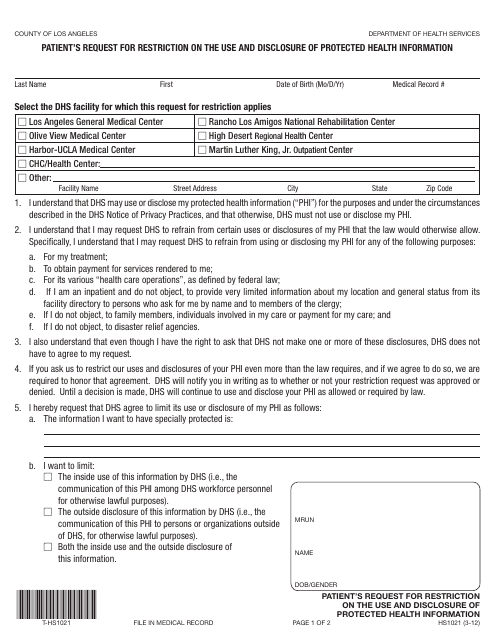
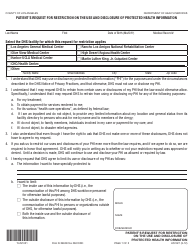
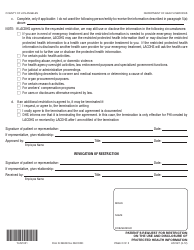
Form HS1021 Patient's Request for Restriction on the Use and Disclosure of Protected Health Information - County of Los Angeles, California
Fill PDF Online
Fill out online for free
without registration or credit card
Download Form HS1021 Patient's Request for Restriction on the Use and Disclosure of Protected Health Information - County of Los Angeles, California
1
2