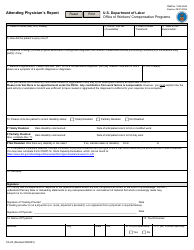
Form CA-17 Duty Status Report
What Is Form CA-17?
This is a legal form that was released by the U.S. Department of Labor - Office of Workers' Compensation Programs on August 1, 2014 and used country-wide. As of today, no separate filing guidelines for the form are provided by the issuing department.
Form Details:
- Released on August 1, 2014;
- The latest available edition released by the U.S. Department of Labor - Office of Workers' Compensation Programs;
- Easy to use and ready to print;
- Yours to fill out and keep for your records;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a fillable version of Form CA-17 by clicking the link below or browse more documents and templates provided by the U.S. Department of Labor - Office of Workers' Compensation Programs.
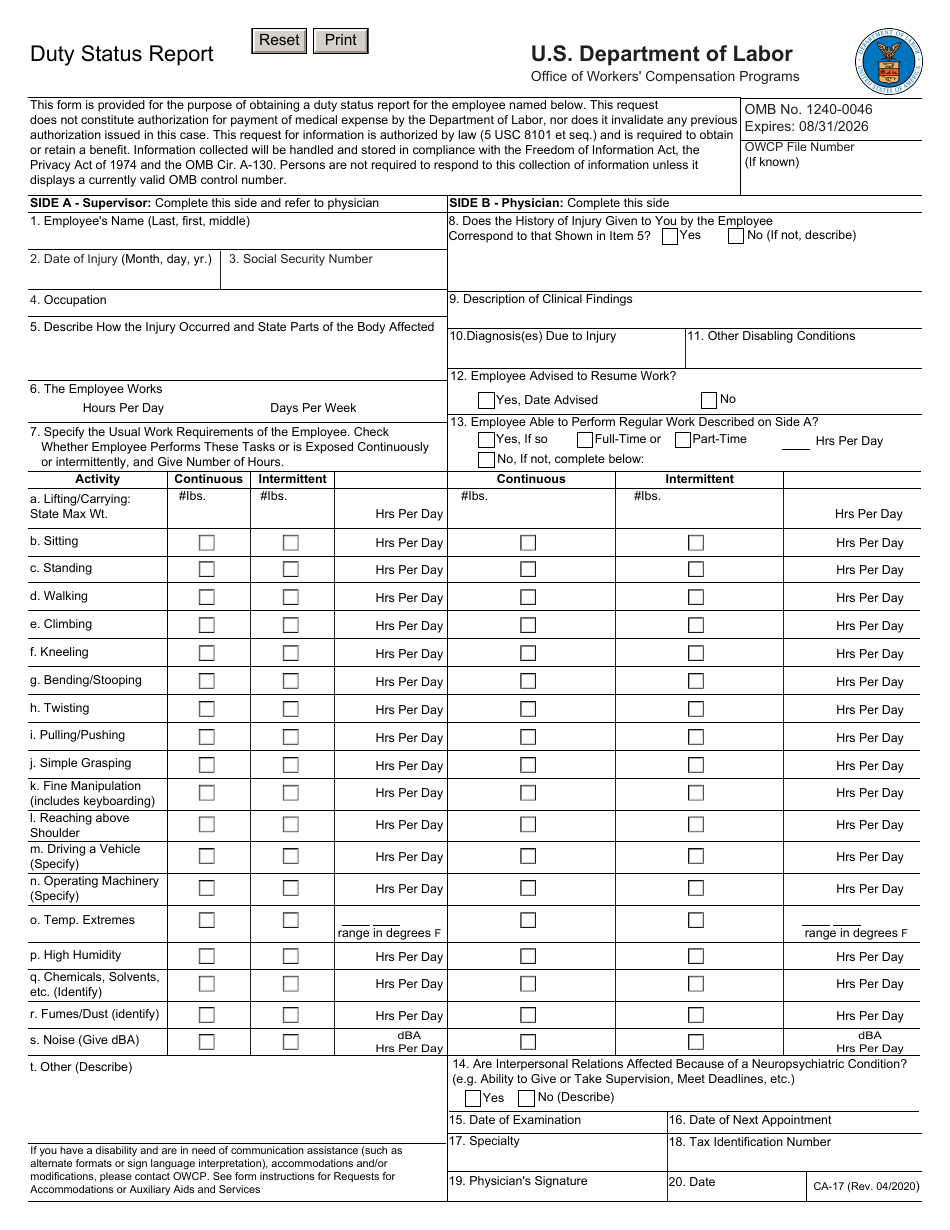
Form CA-17 Instructions
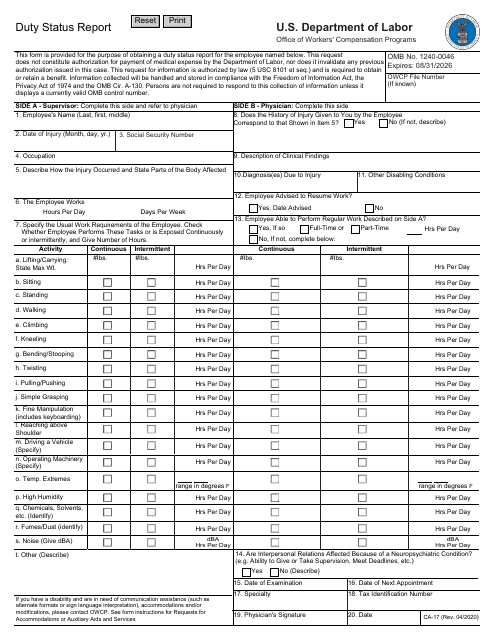
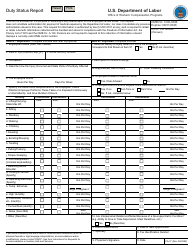
To complete Form CA-17 you will need to complete the following information as the employee's supervisor (Side A):
- General information about the employee (name, social security number, job title);
- How the injury occurred, including the date and parts of the body that were affected by the injury;
- The standard amount of hours worked by the employee in a typical day and week;
- Completion of the checklist of standard job duties performed by employees, including the frequency each of the relevant tasks is performed by the employee in a given day;
- For more specific activities, such as driving a vehicle, operating machinery, or exposure to chemicals, solvents, or noise, additional qualifiers will need to be included;
- This is designed to give the reviewer a complete understanding of the typical work duties of the employee who has filed the Workers' Compensation Report.
Once this form has been completed by the employee's supervisor, it will need to be sent to the physician that examined the employee for the Workers' Claim who will complete Side B:
- Confirmation that the employee has seen the physician for the injuries claimed in Side A;
- Physician's assessment of the injuries and any other injuries that may have been found during the examination process;
- Date recommended when the employee can return to work, or recommendation employee will not be able to return to work;
- Additional section to recommend the employee return to full-time or part-time work, or a maximum number of hours per day;
- Completion of an additional checklist of standard job duties performed by the employee (same as from Side A);
- Final exam information to be completed with the physician's signature and date form was completed.
The physician will need to sign and return the form back to the employee's place of work. Once the employer receives the completed CA-17 Form, it will need to be sent to the following address:
U.S. Department of Labor OWCP/DFEC, PO Box 34090, San Antonio, Texas 78265
Other Revision
Download Form CA-17 Duty Status Report
1
2

3