Florida Agency for Health Care Administration Forms
The Florida Agency for Health Care Administration (AHCA) is responsible for the oversight and regulation of the healthcare system in the state of Florida. Its main goal is to ensure access to quality healthcare services for all Florida residents. The AHCA administers various programs, including Medicaid and the Children's Health Insurance Program (CHIP), and works to implement and enforce healthcare policies and regulations. The agency also provides resources and information to healthcare providers, manages healthcare facilities, and handles complaints and appeals related to healthcare in Florida.
Documents:
39
This document is a sample letter of delegation used in Florida for attestation/certification of reports, data, MPI (Master Plan of Instruction) plans, and other related documents.
This document is used to notify the Florida Agency for Health Care Administration (AHCA) about a change in facility administrator. It is a required form for healthcare facilities in Florida.
This form is used for resident health assessments in assisted living facilities in Florida.
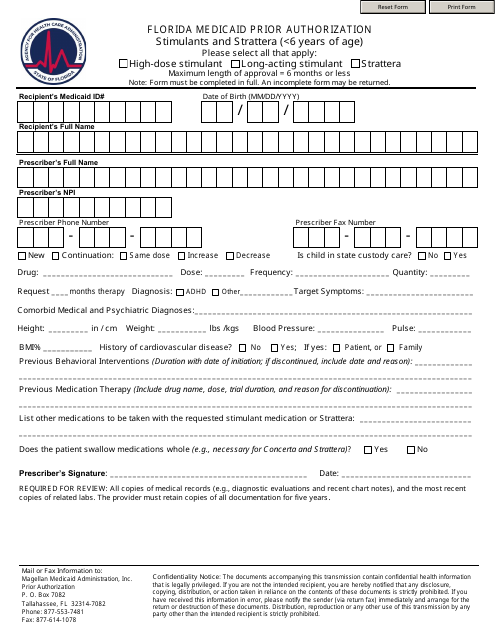
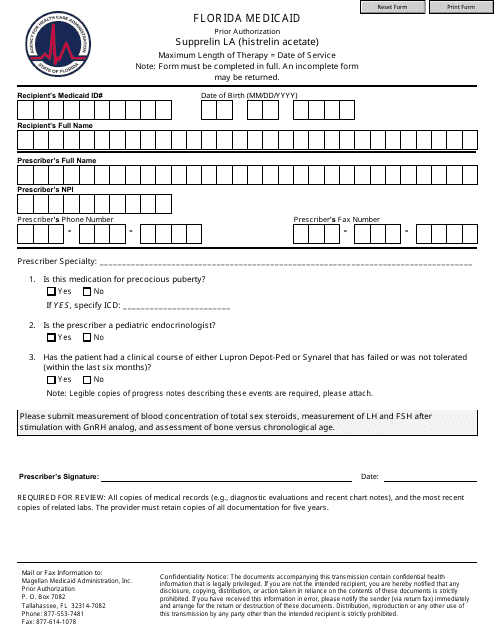
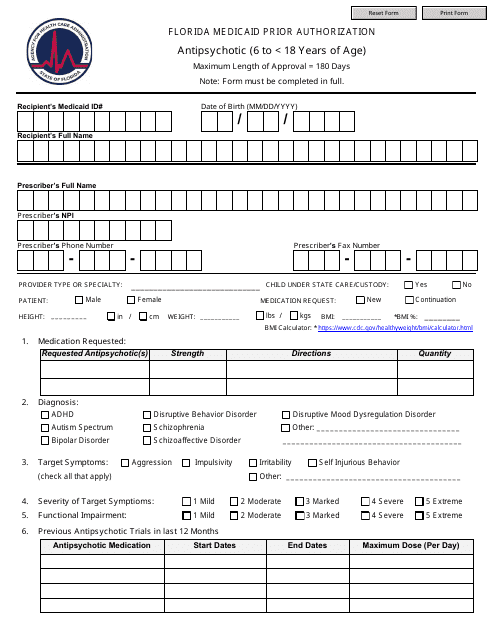
This form is used for requesting prior authorization for antipsychotic medications for children between the ages of 6 and 18 in Florida.
This form is used for reporting the utilization of hospice services in Florida for the first half of the year. It is filled out on a semi-annual basis and provides important data on hospice care in the state.
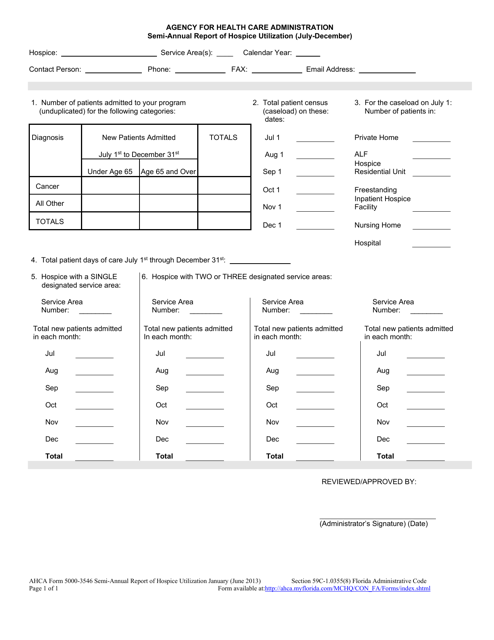
This form is used for reporting the hospice utilization in Florida for the July-December period.
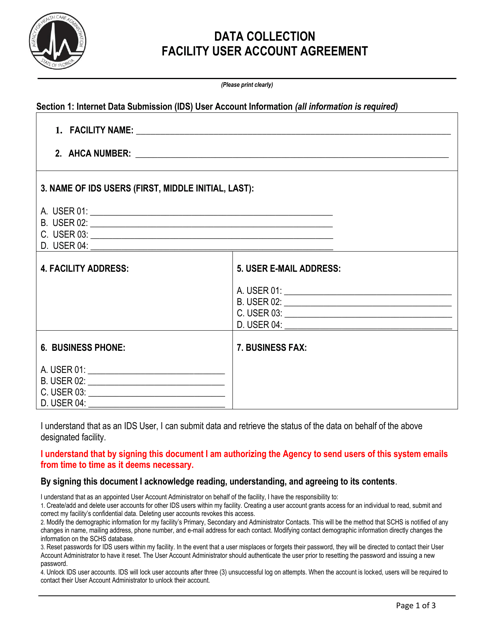
This document outlines the agreement for individuals using facility accounts in Florida. It covers the terms and conditions for accessing and using the facilities.
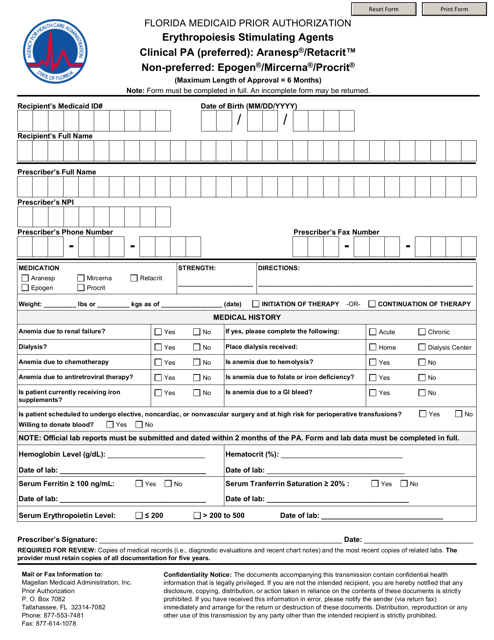
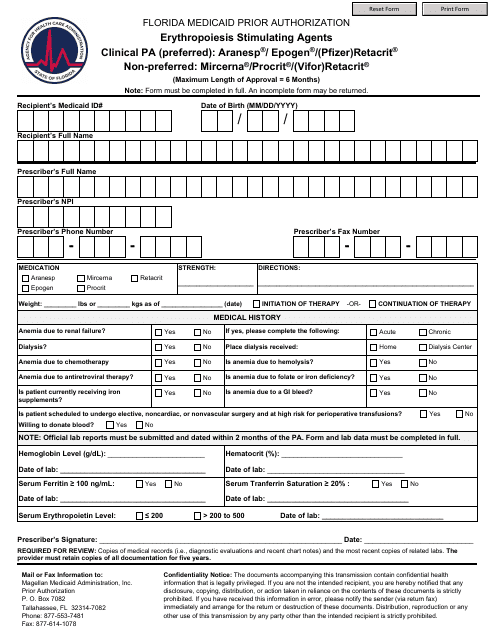
This form is used for obtaining Erythropoiesis Stimulating Agents (ESA) in the state of Florida.
This document is used for verifying HIV diagnoses or providing prophylaxis for HIV in the state of Florida.
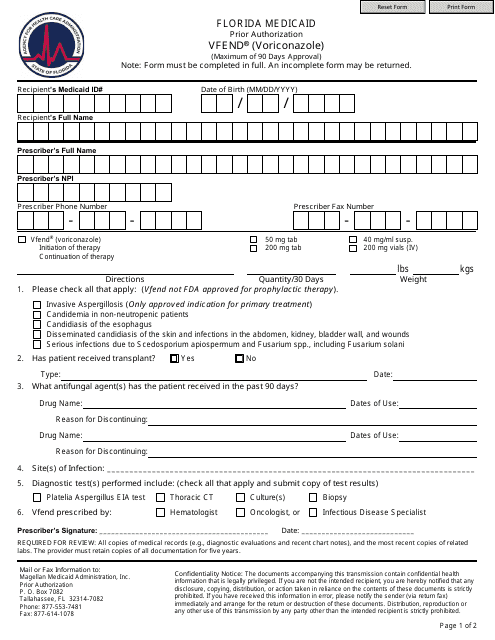
This document is for obtaining prior authorization for the medication Selzentry (Maraviroc) in the state of Florida. It is used to request approval from the insurance company before starting treatment with this medication.
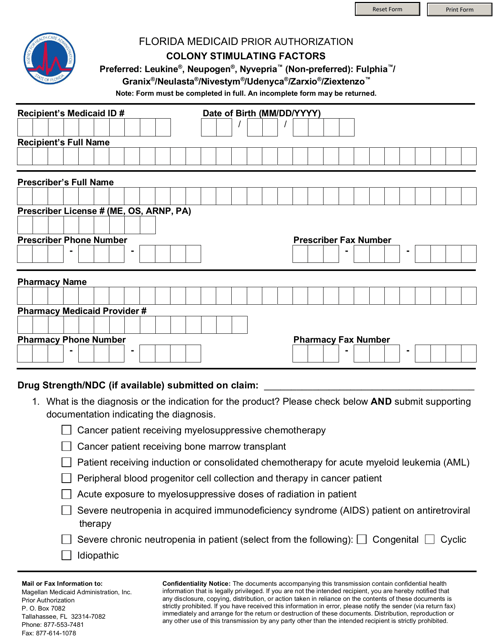
This form is used for Medicaid patients in Florida who need prior authorization for colony stimulating factors.
This form is used for requesting prior authorization for Medicaid coverage of Hepatitis C agents in Florida. It is required to access necessary medications for treating Hepatitis C under the Medicaid program.
This form is used for reporting adverse reactions in organ procurement, tissue banks, and eye banks in the state of Florida.
This form is used for local zoning regulations pertaining to Adult Family Care Homes in Florida. It ensures compliance with the zoning requirements for operating these types of care homes.
This document is used for reporting income and expenses in adult family care homes in Florida.
This Form is used for submitting an application for plan review in the state of Florida under the AHCA (Agency for Health Care Administration).
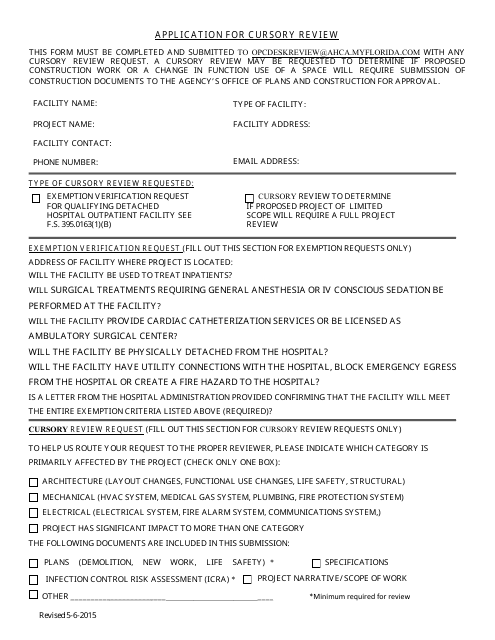
This form is used for applying for a cursory review in the state of Florida. It allows individuals to request a preliminary assessment or evaluation of their case or situation.
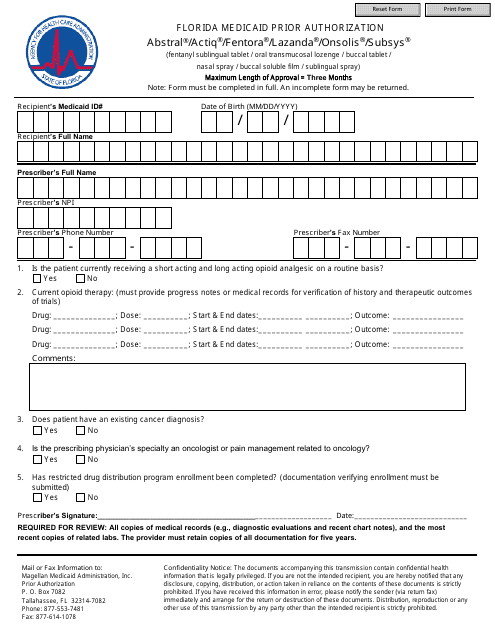
This Form is used for obtaining prior authorization for certain medications (Abstral, Actiq, Fentora, Lazanda, Onsolis, Subsys) under Florida Medicaid. Prior authorization is required to ensure that these medications meet the coverage criteria and are medically necessary for the patient.
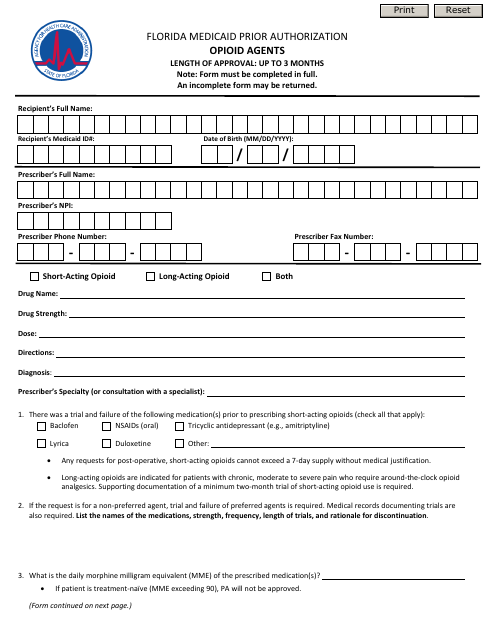
This form is used for obtaining prior authorization for opioid agents under Florida Medicaid in the state of Florida.