Patient Care Templates
Patient Care Documentation - Enhancing the Quality of Healthcare Services
When it comes to providing exceptional patient care, comprehensive documentation plays a crucial role. The patient care documentation, also referred to as medical records, ensures that healthcare professionals have accurate and reliable information about their patients' health and treatment history. This collection of documents, alternately known as patient records or clinical records, encompasses a wide range of forms and questionnaires that facilitate effective communication and continuity of care.
Driven by the aim of improving the quality of healthcare services, these patient care documents serve as a vital resource for healthcare providers. The Oswestry Disability Index Questionnaire Form, for instance, allows healthcare professionals to assess the impact of musculoskeletal conditions on a patient's physical functioning. By utilizing the insights gathered from this questionnaire, healthcare providers can customize treatment plans to meet individual needs.
In emergency situations, the Ambulance Service Questionnaire - Minnesota gathers essential information to ensure swift and appropriate medical attention. This document collection also includes the DSHS Form 13-920 Ocrp Discharge Summary - Washington, a valuable tool in capturing critical details as patients transition from one healthcare setting to another.
Managing chronic conditions effectively is another aspect of patient care, and documents like the Form F-43013 Diabetes Medical Management Plan - Wisconsin enable healthcare providers to monitor and address the specific needs of patients with diabetes. These forms facilitate a collaborative approach to care, empowering patients to actively participate in their treatment plans.
Maintaining patient safety is paramount, and the Form OP-140141B Restraint Medical Flow Sheet - Oklahoma documents any use of restraints, providing valuable information to support safe and responsible practices. Patient care documentation actively contributes to improving patient outcomes and preventing adverse events.
In conclusion, patient care documentation is integral to delivering high-quality healthcare services. These collections of forms, questionnaires, and summaries seamlessly capture vital medical information, promote effective communication, and facilitate collaboration among healthcare professionals. With patient care as the utmost priority, utilizing comprehensive and accurate patient care documentation is essential to enhancing patient outcomes and ensuring the provision of optimal healthcare services.
Documents:
224
This document is a template that healthcare professionals use to create a treatment plan for their patients. It helps outline the goals, interventions, and timeline for the patient's treatment.
This form is used for gathering feedback from patients about their experience at Five Points. It helps the healthcare facility improve its services and address any concerns or suggestions from patients.
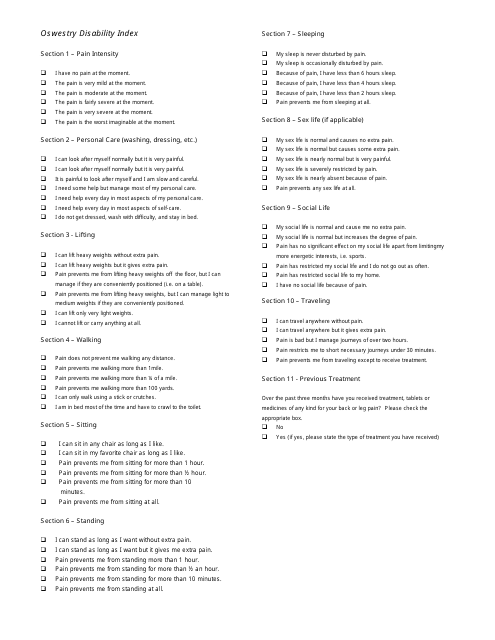
This document is a questionnaire form called the Oswestry Disability Index. It is used to assess the level of disability and pain in individuals with lower back pain. This type of document helps healthcare professionals to determine the impact of back pain on daily activities and develop appropriate treatment plans.
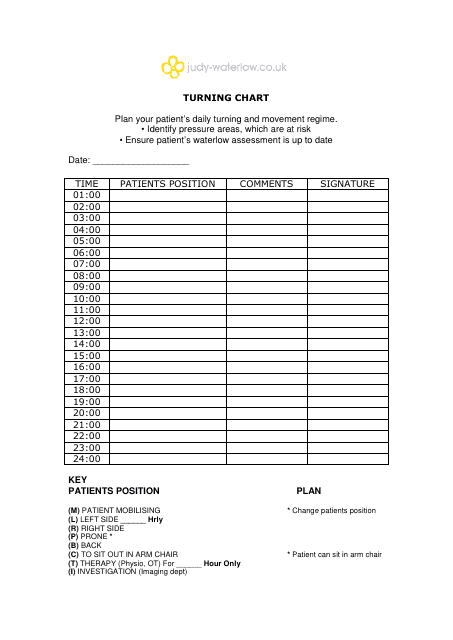
This document is used for tracking and recording the frequency at which patients need to be turned in order to prevent complications associated with immobility.
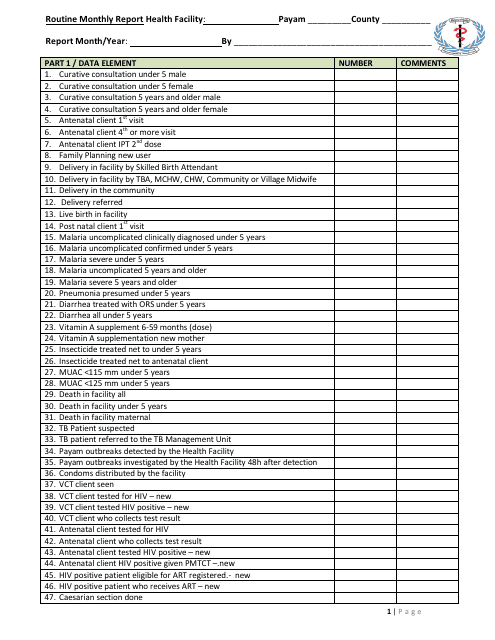
This document is a template for health facilities to report their monthly activities and statistics. It helps in monitoring the performance and progress of the facility.
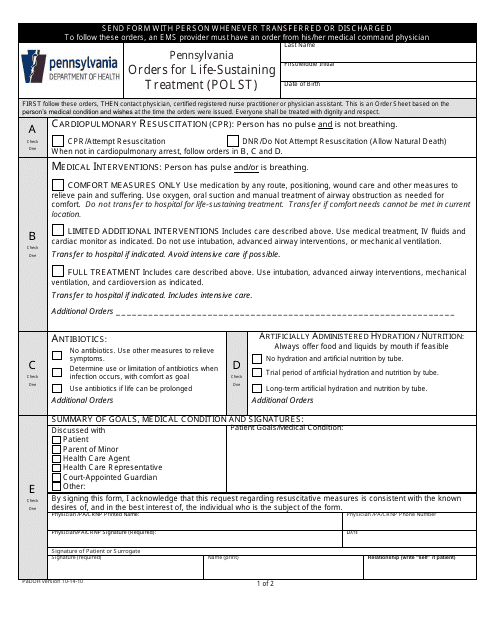
This document is used in Pennsylvania to record a person's end-of-life medical treatment preferences. It helps ensure that individuals receive the life-sustaining treatment they desire.
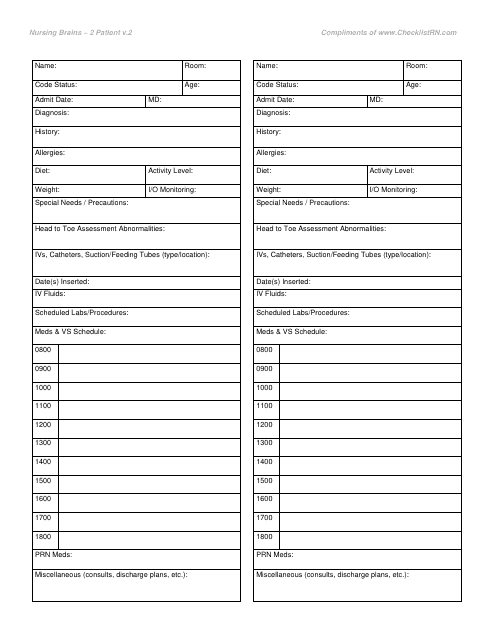
This Form is used for recording and sharing information about patients in a hospital. It helps nurses organize and communicate important details about the patients' conditions, treatments, and medications.
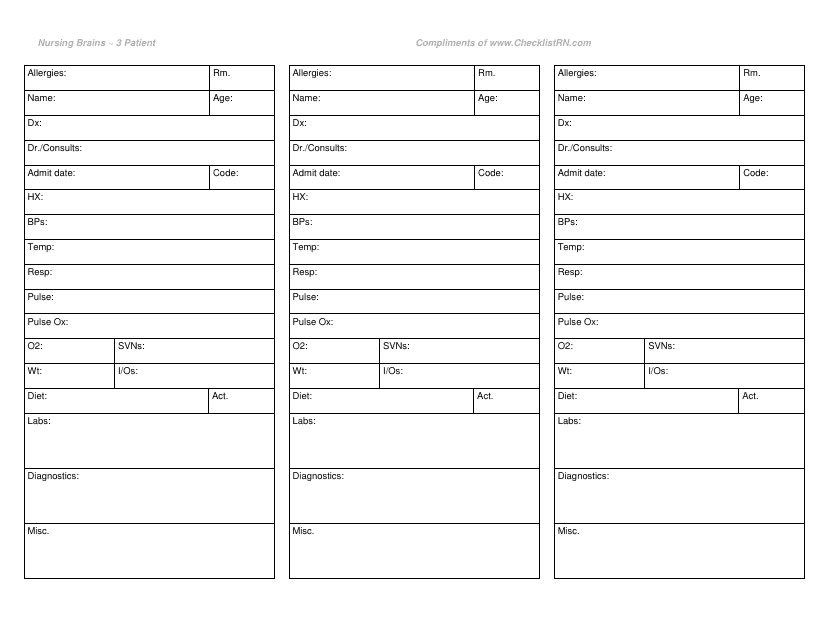
This form is used for organizing patient information in the nursing field. It is designed to help nurses keep track of important details for up to three patients.
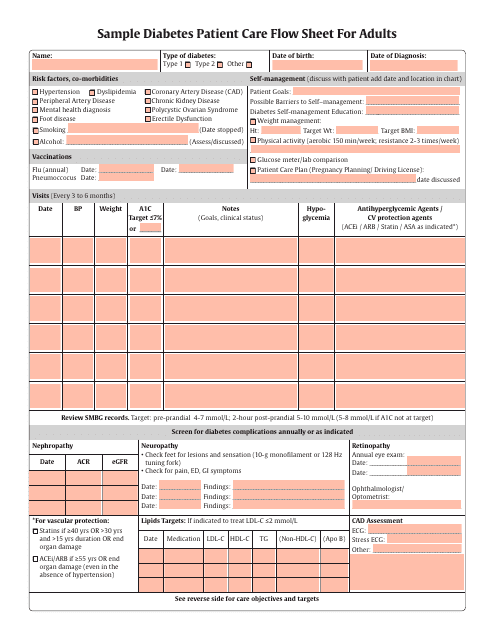
This type of document is a sample flow sheet used for tracking and documenting the care and treatment of adult diabetes patients. It helps healthcare professionals monitor and manage their patients' condition effectively.
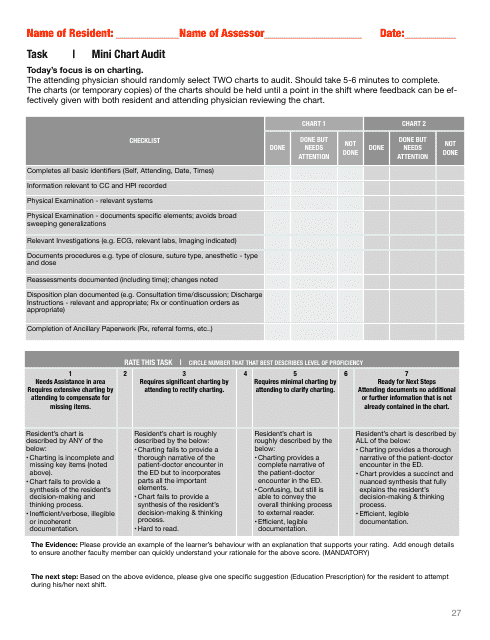
This document is a template for conducting mini audits on charts. It helps ensure accuracy and completeness of chart information.
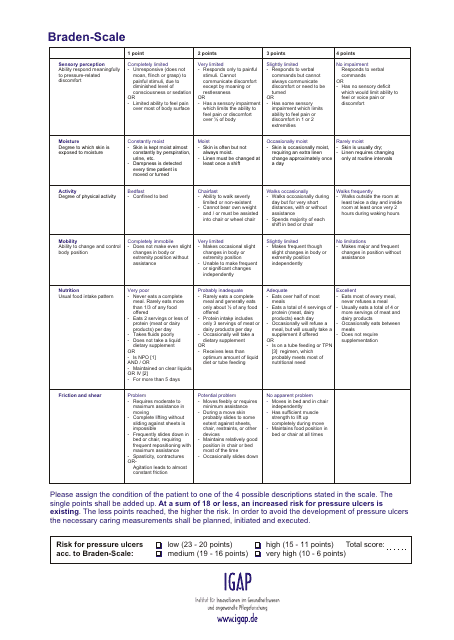
This document is a Braden Scale Chart used for assessing a patient's risk for developing pressure ulcers. It helps healthcare professionals determine the appropriate preventative measures and interventions needed to prevent skin breakdown.
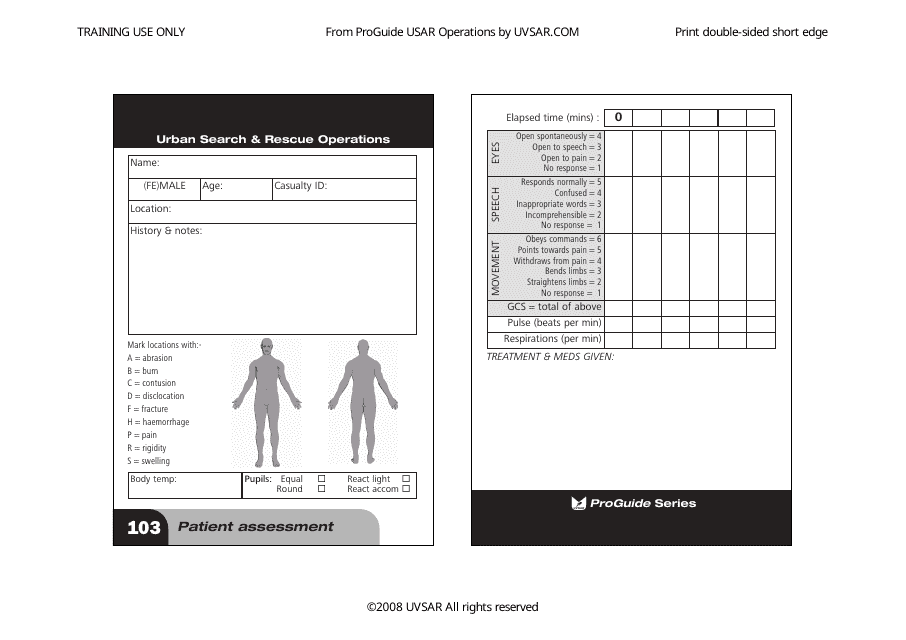
This document is used for assessing the condition and needs of a patient. It helps healthcare professionals gather information about the patient's medical history, symptoms, and current health status.
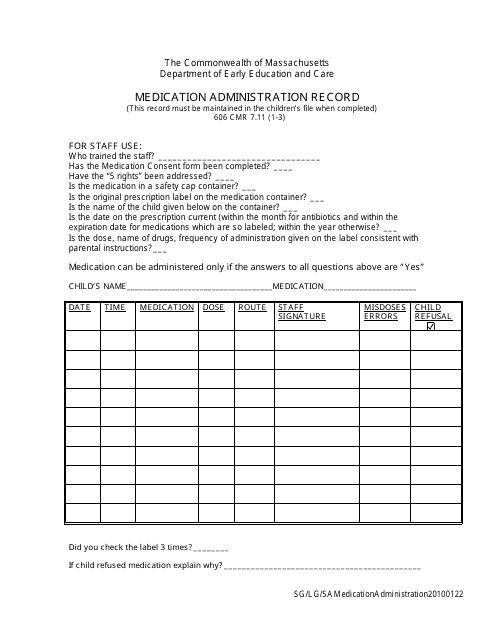
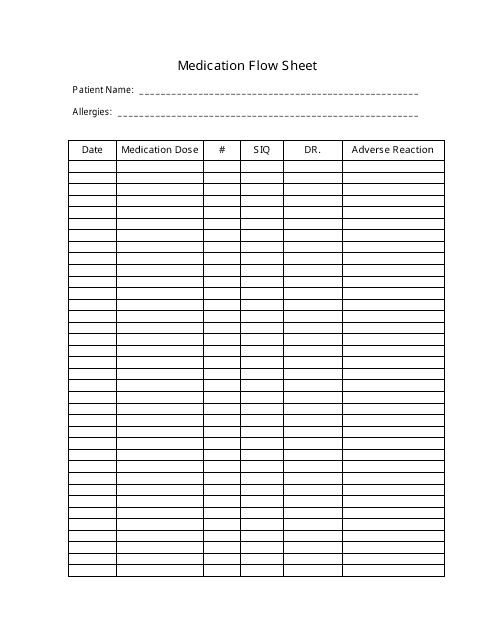
This document is used to record the administration of medication in the state of Massachusetts. It helps to track and monitor medication doses given to individuals.
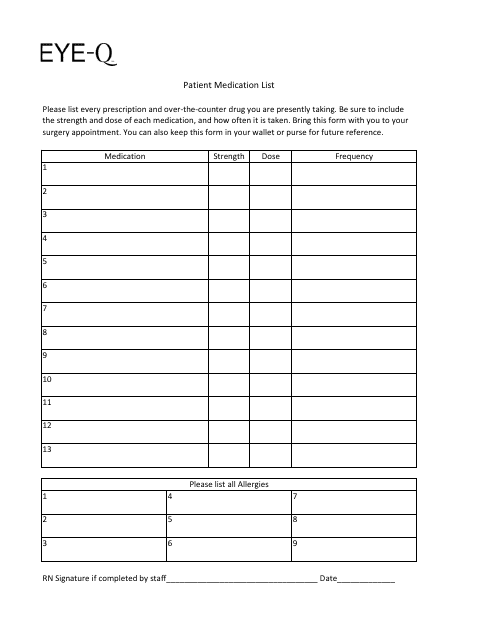
This form is used for creating a list of medications that the patient is taking specifically for Eye-Q purposes. It helps keep track of the patient's eye-related medications.
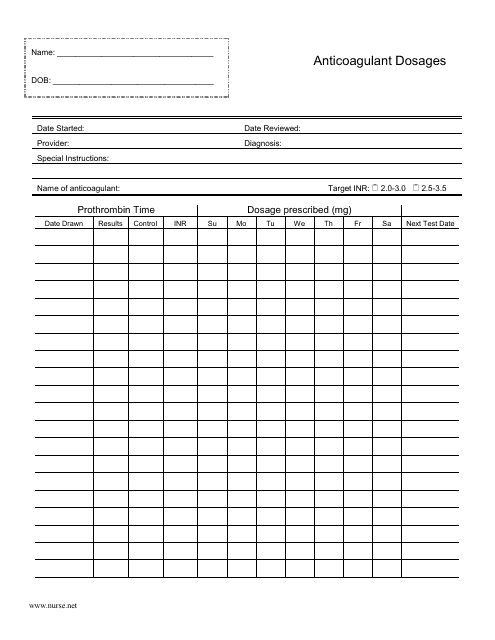
This document is used to track and record the dosage of anticoagulant medications for patients.
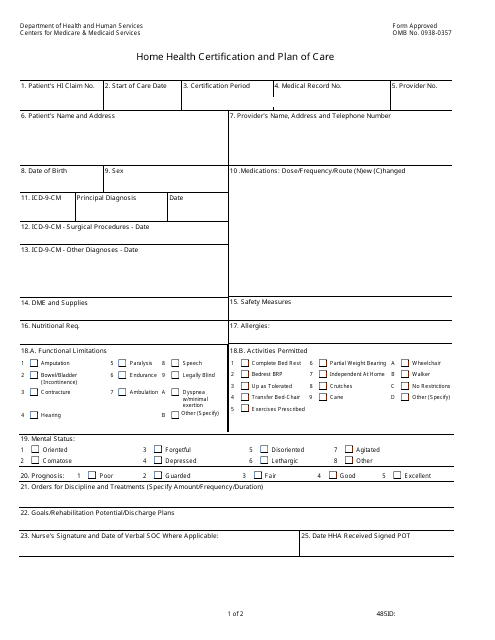
This form is filled out by the patient's attending physician and used as a fiduciary document in order to authorize professional health services.
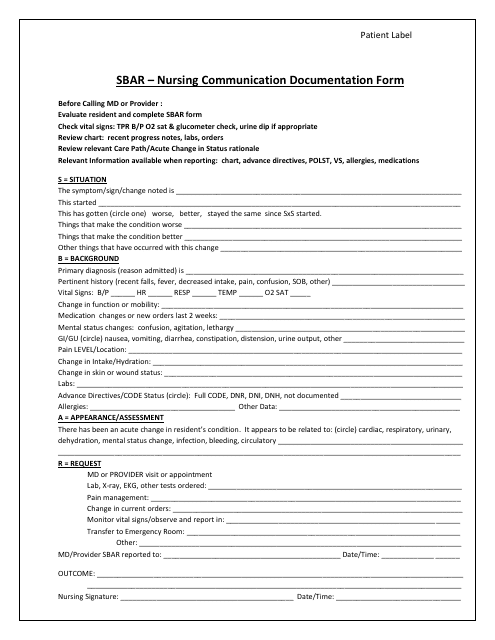
This form is used for documenting communication between nurses and patients, including important information about treatments, medications, and patient care. It helps ensure clear and accurate communication among healthcare providers.
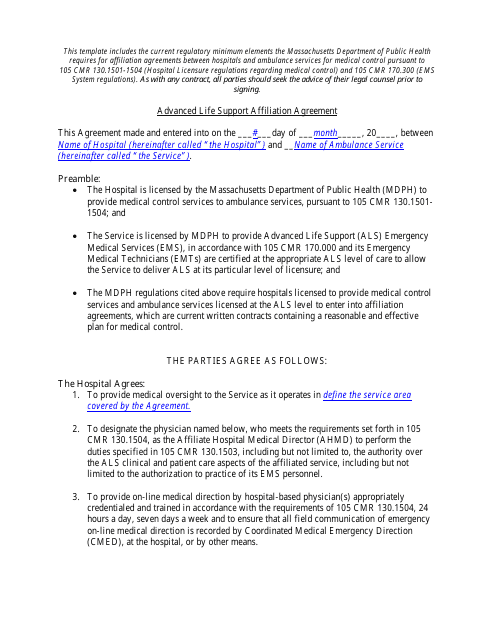
This document is a template for an agreement between two organizations for an affiliation related to advanced life support. It provides a framework and terms for collaboration in providing advanced life support services.
A Nursing Report Sheet is a document that should be completed by medical professionals to provide details for nursing their patients.
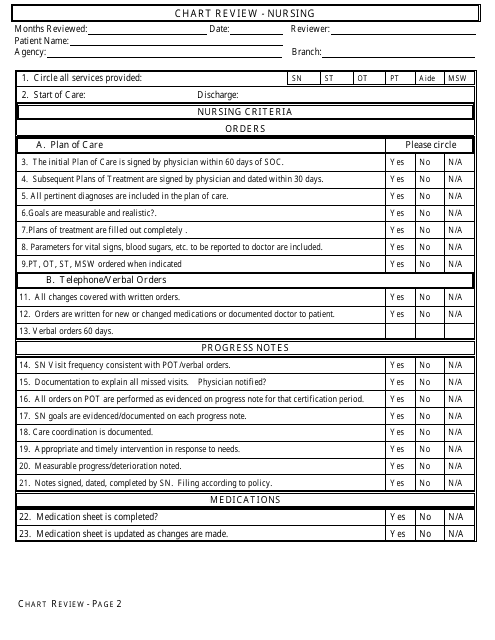
This document template is used for reviewing nursing charts. It helps ensure accurate documentation and proper patient care.
This type of document is used for conducting triage on unscheduled patients in emergency situations.
This document is used for administering oxygen to individuals in need of medical assistance. It provides instructions on how to safely and effectively administer oxygen therapy.
This document is used for managing an intravenous infusion.
This form is used for delineating clinical privileges in the field of pathology. It helps to define the specific privileges that a healthcare provider has regarding pathology services.
This form is used for reporting public health nursing activities. It is used to document various nursing activities and provide a record of services provided.
This form is used for managing a seizing patient.
This form is used for documenting nursing notes in a patient's medical record.
This Form is used for obtaining approval for medical care under the VHA Choice program.
This form is used for documenting a doctor's orders and treatment plan. It provides instructions for medical staff and ensures proper patient care.
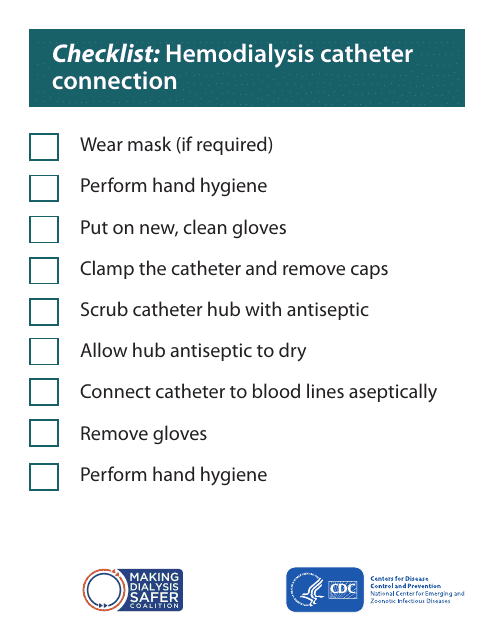
This document is a checklist for ensuring proper connection of a hemodialysis catheter. It provides steps and guidelines to follow to ensure a secure and proper connection.
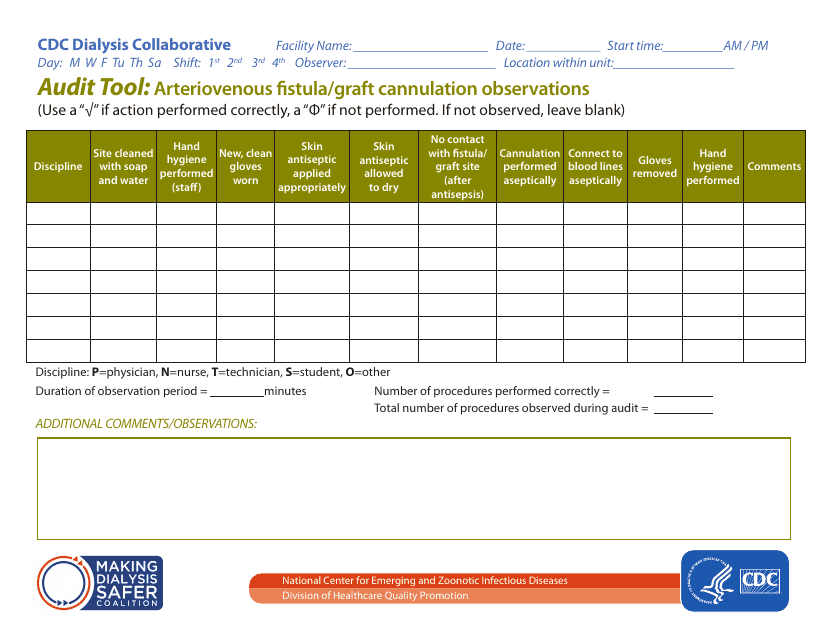
This document is an audit tool used to record observations related to the cannulation of arteriovenous fistulas or grafts. It helps ensure proper and safe cannulation procedure.
This form is used for applying for Chronic Dialysis Service in California.
This document is used for creating a shared plan of care for healthcare providers in Colorado. It helps coordinate and communicate the patient's care among various providers.
This document is used to assess the risk for impaired skin integrity in the state of Alabama. It helps healthcare professionals identify individuals who may be at risk for developing skin problems and implement appropriate preventive measures.
This form is used for requesting a long-term care bed reserve or reporting a temporary absence for individuals in Illinois.
