Nursing Report Sheet Template
What Is a Nursing Report Sheet?
A Nursing Report Sheet is a document that should be completed by medical professionals to provide details for nursing their patients. This document contains all of the necessary information about the nursing activity regarding a particular patient, such as the patient's assessment, changes in their condition and progress notes, the treatment they have received, and any clinical investigations. A nurse may also include a plan of care in this report.
Alternate Name:
- Nurse Report Sheet.
A Nurse Report Sheet allows the quick understanding of patient information, helps the nurse make a treatment plan, and determines what procedures they have to perform during their shift. In addition to the indicated functions, this report may be used by a nurse to defend their interests in court and evaluate their nursing care in the nursing management system. This document simplifies communication between professionals of the healthcare team. A Nursing Report Sheet PDF version can be downloaded through the link below.
How to Make a Nursing Report Sheet?
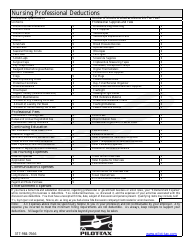
A Nursing Report Sheet contains standardized medical codes, known to all medical professionals. The usage of these codes facilitates the process of providing the necessary information to other nurses and makes the report more concise, clear, and informative.
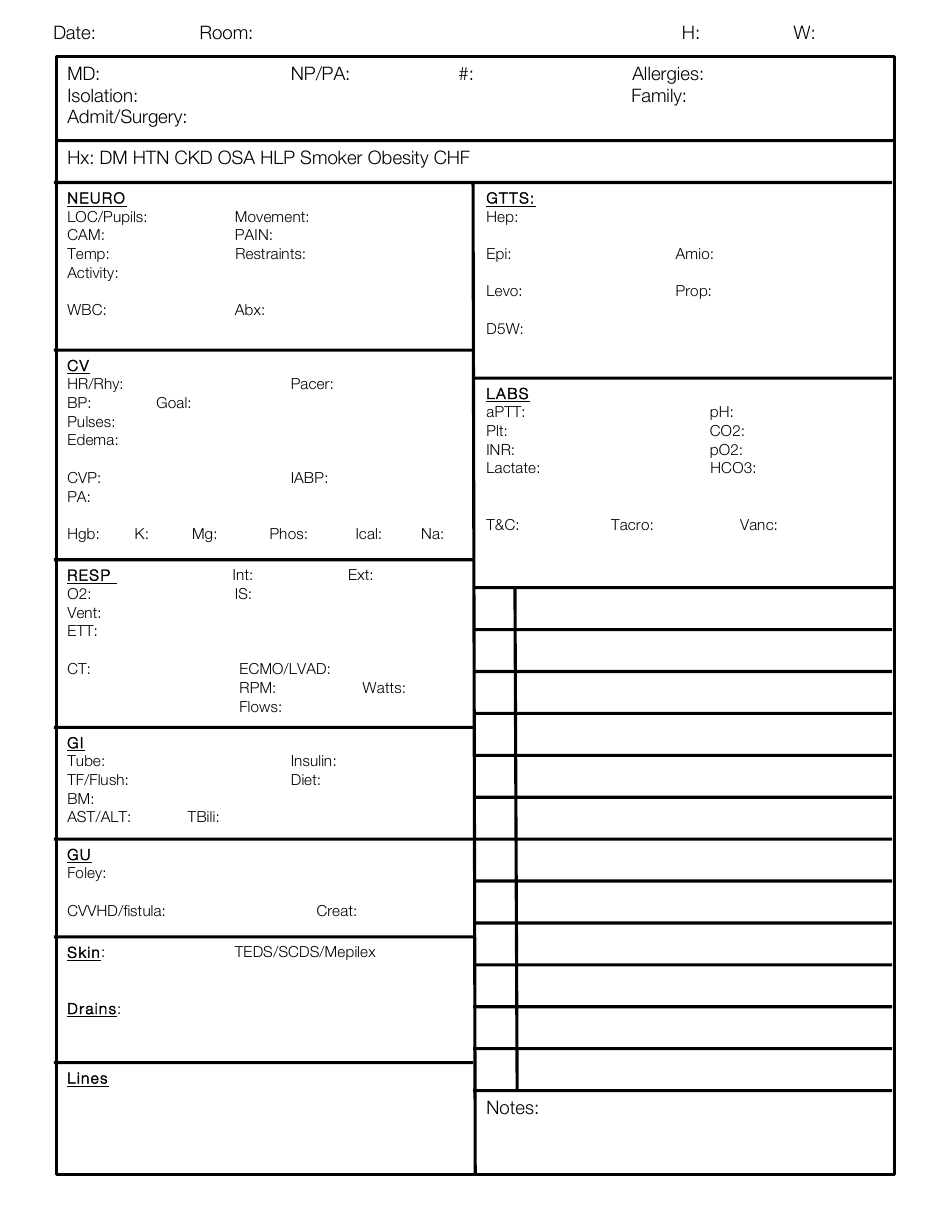
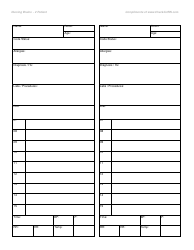
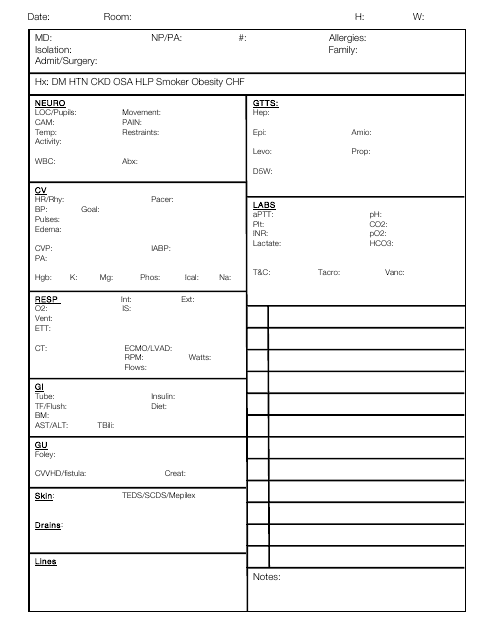
A Nursing Report Sheet template must be filled in as follows:
-
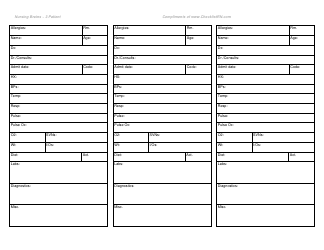
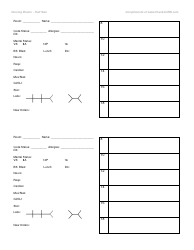
The applicant should enter the date of completion. Indicate the room number, and specify the height and weight of the patient.
-
The applicant must enter information about the medical professionals treating this patient. In the MD section, indicate the name of a medical doctor, in the NP/PA section, enter the name of a nurse practitioner or physician assistant. Provide information about allergies of the patient.
-
In the Hx section, the applicant should indicate the medical history of this person. Choose the code reflecting relevant medical conditions or past incidents.
-
Fill in detailed information about the functioning of body systems of the patient:
- Neuro . Specify information about the neurologic system. Estimate the equality of the pupils and their reaction to light, compare the size and reactivity of each pupil. Estimate activity, movement, and restraints of the patient. Measure and enter body temperature;
- CV . Fill in details about the cardiovascular system of this person. Enter their pulses, edema, and information about the usage of a pacer;
- RESP . Complete information about the functioning of their respiratory system;
- GI . Fill in details about the gastrointestinal system of the patient. Provide information about the usage of the tube, enter the AST/ALT ratio, and insulin coverage. Specify the recommended diet;
- GU . Fill in details about their genitourinary system. Provide information about the usage of the Foley catheter;
- Skin . Describe the skin of the patient and provide information about the usage of thromboembolic deterrent stockings (TEDS) and sequential compression devices (SCDs);
- LABS . Provide information about the results of laboratory analysis, enter aPTT, INR, lactate ratio and others;
- The form has some additional space for notes and recommendations.
To track the condition of patients regularly, a nurse should start completing a Nurses Report Sheet at the beginning of their shift and make records there, taking into account information contained in the previous employee's report. This nurse should also pass the completed report to the medical specialist who will work after them.
Looking for something else? Check out these related files: