OCA Official Form 960 Authorization to Release Health Information Pursuant to Hipaa - New York
What Is OCA Form 960?
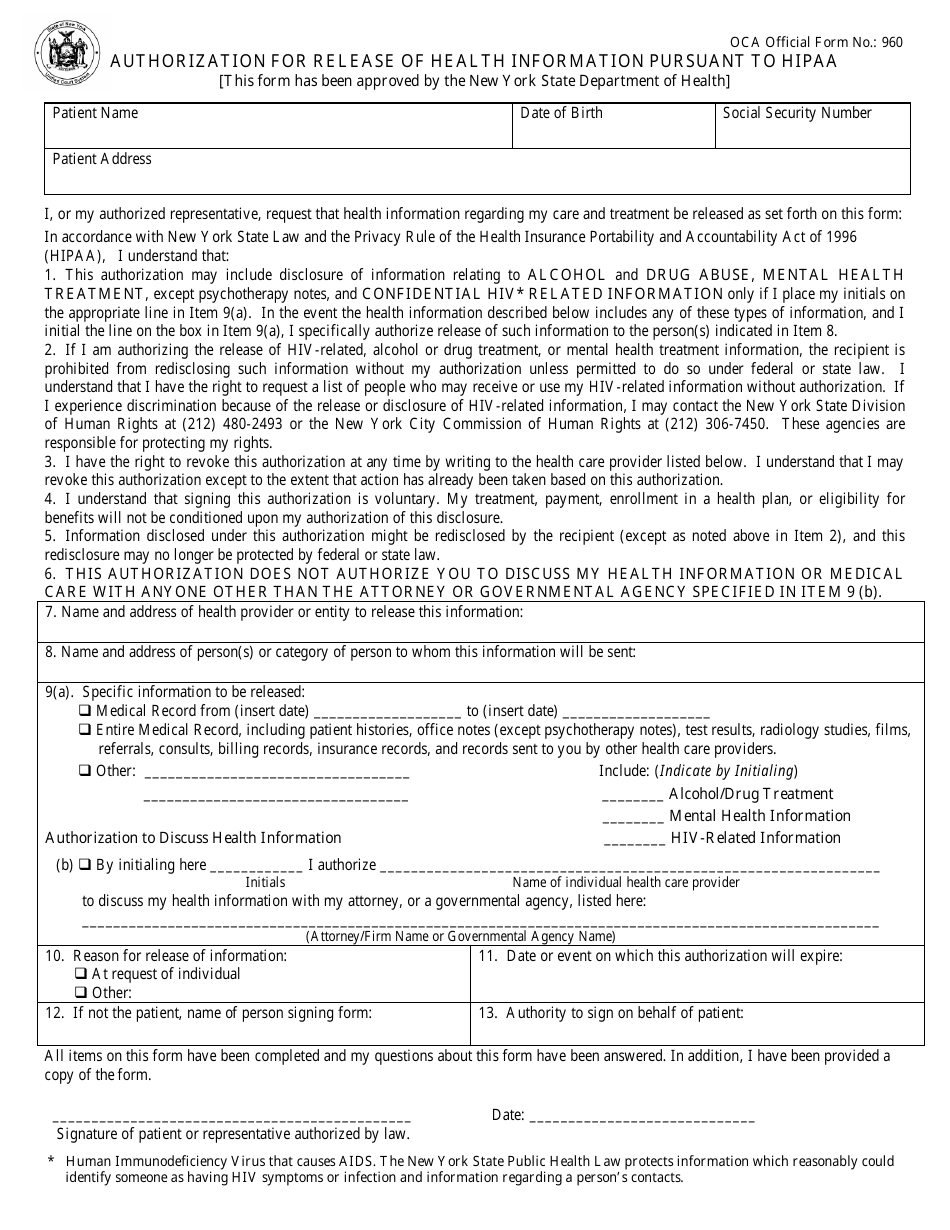
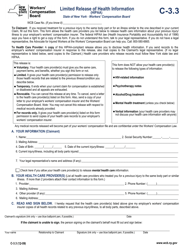
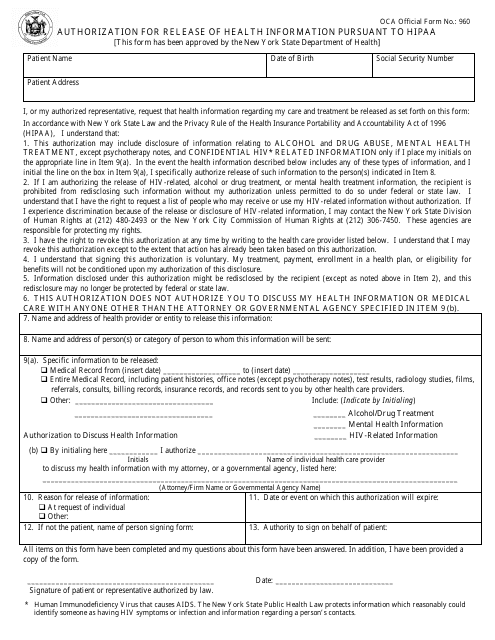
OCA Form 960, Authorization to Release Health Information Pursuant to HIPAA , is a legal document signed by a patient that gives consent to the release of health information within the state of New York. This document gives permission to use protected health information for certain purposes - treatment, payment, and operations, and disclose protected health information to third parties specified by the patient. It ensures the protection of the patients' privacy and allows health data to flow freely between authorized parties for healthcare activities.
Alternate Name:
- OCA Official Form 960.
If you are seeking your own medical records or wish to give another individual or agency permission to do so on your behalf, complete OCA Official Form 960.
This form was released by the New York State Office of Court Administration . It has replaced Form MAP-751D (Authorization for Disclosure of Health Information) on . You can download an OCA Form 960 fillable version through the link below.
How to Fill Out OCA Official Form 960?
Include the following information in the OCA Official Form 960 to request the release of health information:
-
Write down the name and address of the patient, date of birth, and social security number;
-
In accordance with the Health Insurance Portability and Accountability Act (HIPAA), a patient must understand the following:
- You disclose information relating to drug and alcohol abuse, mental health treatment, and HIV-related information;
- The recipient of the information cannot redisclose it without your authorization. You have the right to request a list of individuals who may receive and use your HIV-related information without authorization. Your rights are protected by the New York State Division of Human Rights and the New York City Commission of Human Rights;
- You may revoke this authorization at any time;
- You sign the authorization voluntarily and your treatment and enrollment in health plans cannot be conditioned upon this authorization;
- Your health information may be redisclosed by the recipient if you specifically authorize it;
- You only authorize the recipient to discuss your health information with the attorney or governmental agency indicated in the OCA Form 960;
-
Provide the name and address of the health provider or entity who is authorized to release this information;
-
Name the individual to whom this information must be sent;
-
State which information can be released - your medical records from a certain period of time, entire medical records, and information regarding your alcohol or drug treatment, mental health information, or HIV-related information;
-
Authorize the individual health care provider to discuss your health information with your attorney, or a governmental agency. Name the attorney or agency;
-
Select the reason for the release of information;
-
Specify the date or event on which the authorization has to expire;
-
Name the preparer of the form and indicate the authority to sign on behalf of the patient;
-
Sign and date the form.
Download OCA Official Form 960 Authorization to Release Health Information Pursuant to Hipaa - New York
1

2