![]() This version of the form is not currently in use and is provided for reference only. Download this version of
DD Form 2870
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
DD Form 2870
for the current year.
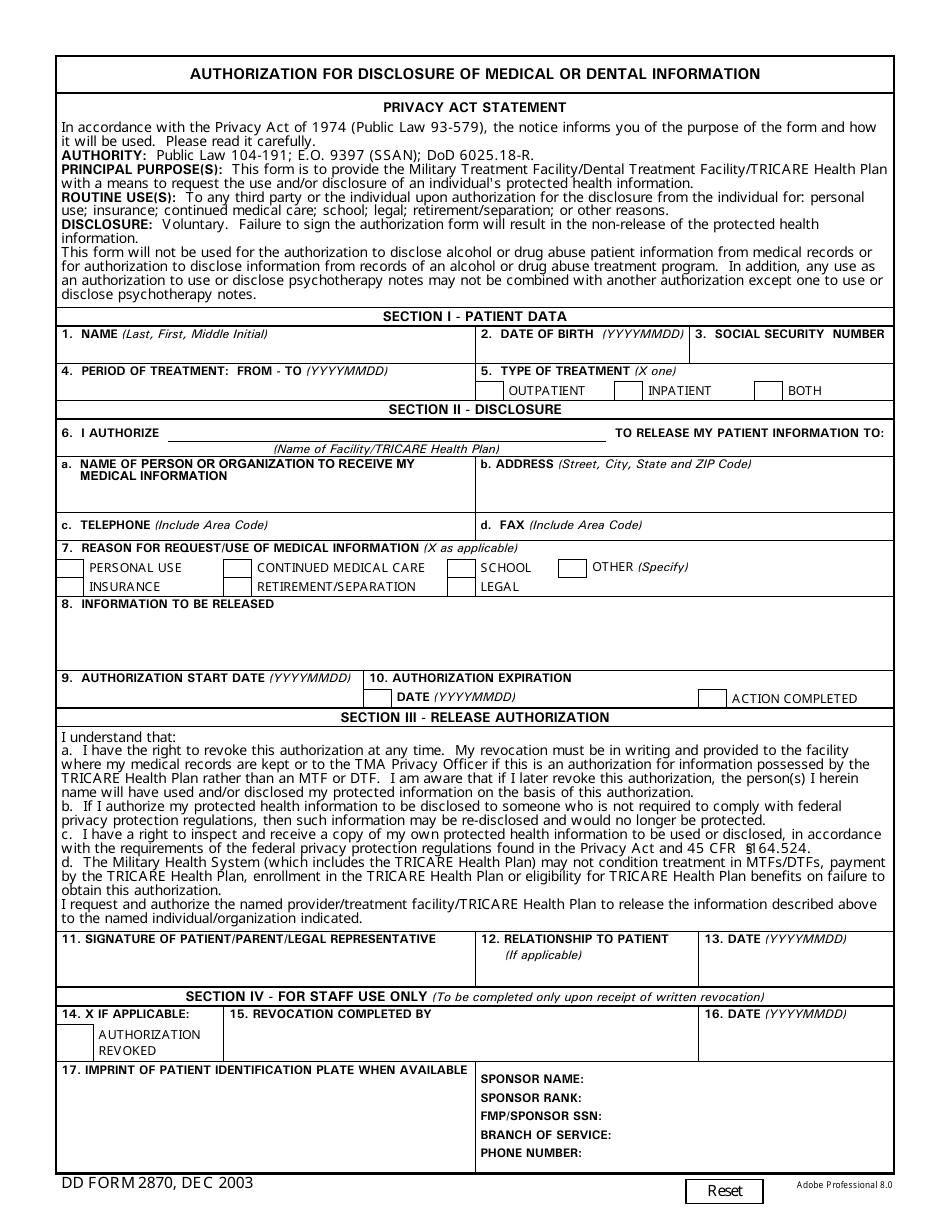
DD Form 2870 Authorization for Disclosure of Medical or Dental Information
What Is DD Form 2870?
DD Form 2870, Authorization for Disclosure of Medical or Dental Information, is used to permit the health care provider to disclose personal medical information to the third party for legally justified purposes.
The latest edition of this form - often incorrectly referred to as the DA Form 2879 - was released by the Department of Defense (DoD) on December 1, 2003 . A fillable up-to-date Form DD 2870 is available for download and digital filing below or can be supplied through the Executive Services Directorate website.
DD Form 2870 cannot be applied for authorization to reveal drug or alcohol abuse records, as well as alcohol or drug abuse treatment. Filling and signing this form is completely voluntary and authorization can be revoked anytime.
DD Form 2870 Instructions
- Section I contains the ID information of the person requesting disclosure. This section also includes the period and type of treatment being revealed. To reveal all medical records, use the day entering the military as a starting point.
- State the facility or TRICARE Health Plan authorized to disclose patient data and the organization to receive it in Section II. Check the reason for the release and briefly specify the information to be disclosed. Finally, state the authorization start and expiration dates.
- Section III requires the patient's signature and the date. If they are unable to sign, the legal representative can do this. In this case, the form must be submitted with a document confirming the representatives' authority.
- Section IV should be left blank. It is filled by the staff in case of revocation.
DD 2870 Related Forms:
- TRICARE for Life Authorization to Disclose Information gives the permission to your TRICARE for Life contractor to disclose the protected health information (PHI);
- TRICARE Overseas Authorization to Disclose Information provides the authority to the TRICARE Overseas Program contractor to release your protected health information;
- Active Duty Dental Program Request and Authorization for Disclosure of Health Information authorizes the disclosure of health data between spouses, for children 18 years and older or other individuals not allowed to receive PHI without written permission.