Form SSA-789 Request for Reconsideration - Disability Cessation Right to Appeal
What Is Form SSA-789?
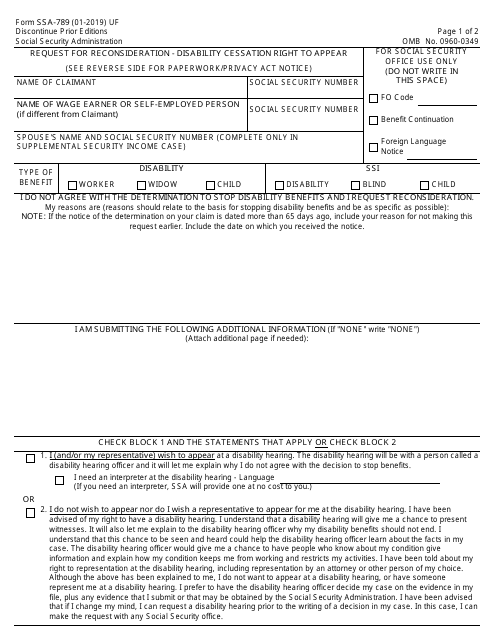
Form SSA-789-U4, Request for Reconsideration - Disability Cessation , is a form used for filing requests to reconsider cessation of disability benefits. The form was issued by the U.S. Social Security Administration (SSA) with the latest version of the document released on January 1, 2019 . An SSA-789 fillable form is available for download and digital filing below.
Alternate Names:
- Form SSA-789;
- SSA Request for Reconsideration Form.
If the SSA decides that you are no longer eligible to receive your Social Security disability benefits, they will notify you about the termination of your payments. However, in most cases, you have the right to appeal this decision. The right to appeal depends on the reason your benefits were terminated. To initiate the appeal, you need to submit the SSA Request for Reconsideration Form. If you want to continue receiving your benefits during the appeal process, fill out and submit Form SSA-789 within 10 days since you received the termination notice. In general, you have 60 days from the date you received the notification to submit the form and initiate the appeal.
What Is the Difference Between Form SSA-561 and Form SSA-789?
Form SSA-561-U2, Request for Reconsideration, is the document that allows you to ask the SSA to reconsider the decisions they made regarding your benefits. These decisions may include denial of disability benefits, eligibility for special veteran benefits, and recalculation of your benefits. This form is usually filled out to appeal the initial claim while Form SSA-789 is used to appeal the decision to stop the disability benefits that were paid for some time.
How to Fill Out Form SSA-789?
The document consists of two pages. It takes about 13 minutes to complete the SSA Request for Reconsideration Form. This includes reading the instructions, gathering all the required data, and answering the questions.
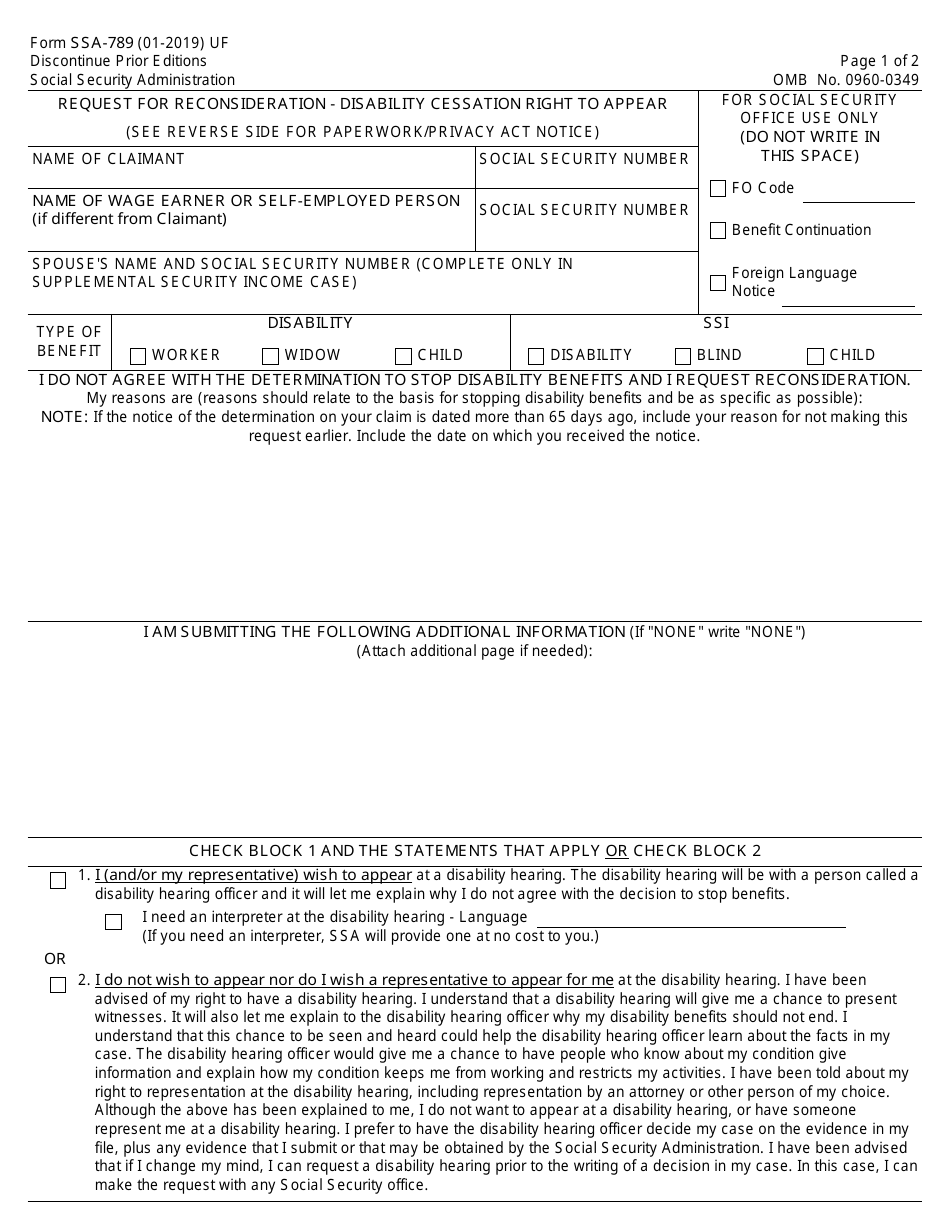
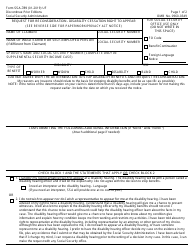
- Provide the name of the claimant exactly as shown on the cessation notice. Specify the Social Security number (SSN) of the claimant.
- If the claim number holder is different from the claimant, provide the applicable name and SSN in the next lines. Always indicate the claimant's SSN first, even if it is not the claim number.
- In case of supplemental security income, provide the name and the SSN of your spouse.
- Choose the type of benefits you ceased to receive.
- Provide the reasons you request the reconsideration of your entitlement. Be as specific as possible. If the termination notice was issued more than 65 days ago, provide the reason why you did not submit your claim earlier. Specify the date you received the termination notice.
- Specify the additional information you submit. If you do not submit any additional information, enter "None." If the space provided is not enough, attach additional sheets.
- Choose if you wish to appear at your disability hearing. You may designate a legal representative to appear for you. If you need an interpreter at the hearings, check the applicable box, specify your language and the SSA will provide you one for free.
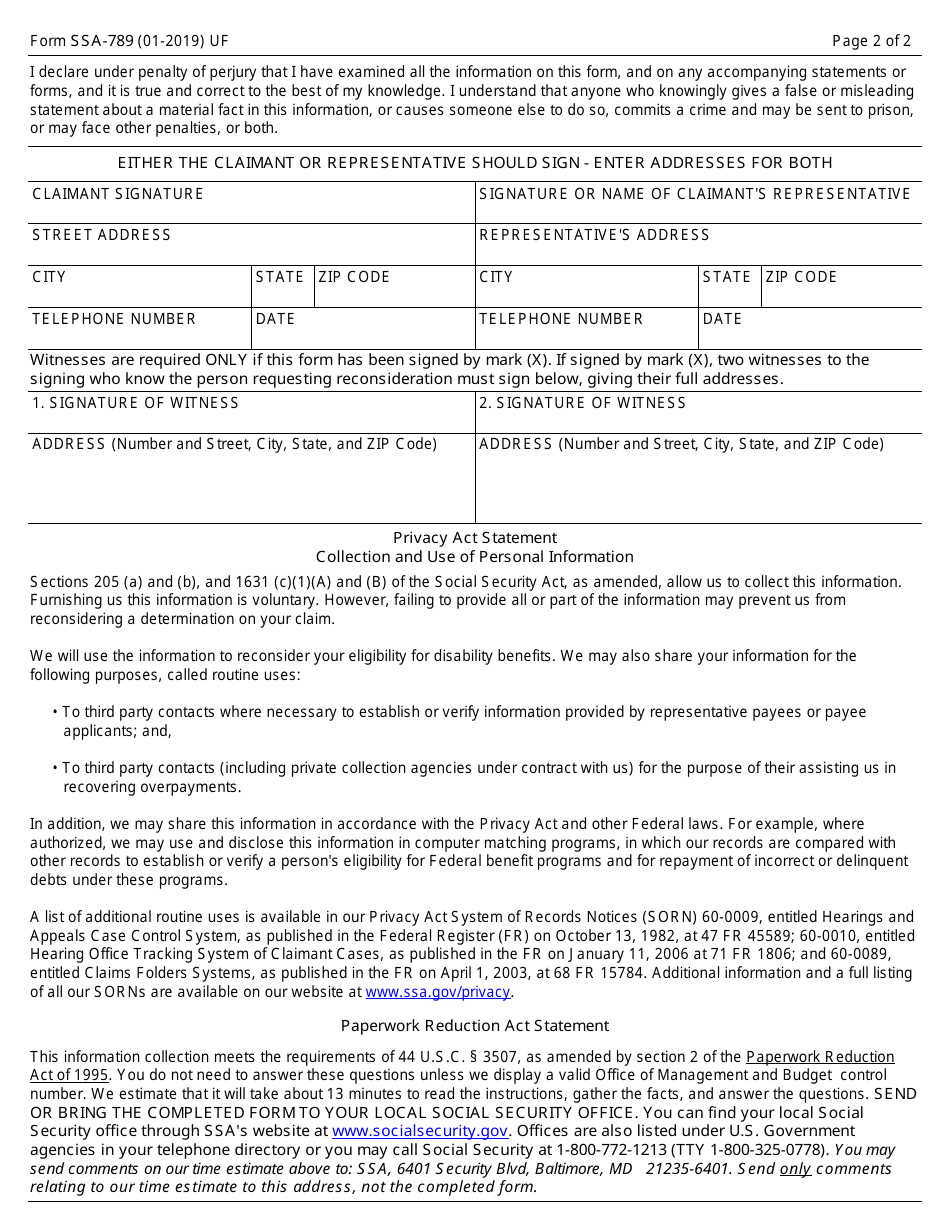
- The document should be signed either by the claimant or by a legal representative.
- If the form is signed by the representative, it is still necessary to provide the full mailing addresses for both, the representative and the claimant.
- If you signed the document with an "X," ask two impartial witnesses who know you to sign the document and to provide their mailing addresses.
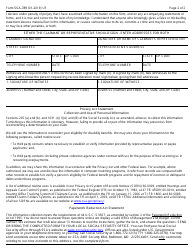
Where to Mail Form SSA-789?
Mail or take the completed form to your local Social Security office. The full list of the offices is provided at the SSA official website. You can also find the applicable office in your telephone directory under U.S. Government agencies or by calling the SSA phone number indicated on the form.
Download Form SSA-789 Request for Reconsideration - Disability Cessation Right to Appeal
1
2