Form DOH-4359 Physician's Order for Personal Care / Consumer Directed Personal Assistance Services - New York
What Is Form DOH-4359?
Form DOH-4359, Physician's Order for Personal Care/Consumer Directed Personal Assistance Services , is a document that can be used by individuals who would like to apply for certain types of assistance such as home care, help with skilled or personal tasks, housekeeping, etc. The purpose of the document is to collect information about an individual who, due to their health condition, needs help in performing various tasks. This form is supposed to be completed by a physician.
The Physician's Order for Personal Care Form was issued by the New York State Department of Health and was last revised on January 1, 2010 . Form DOH-4359 is available for download below.
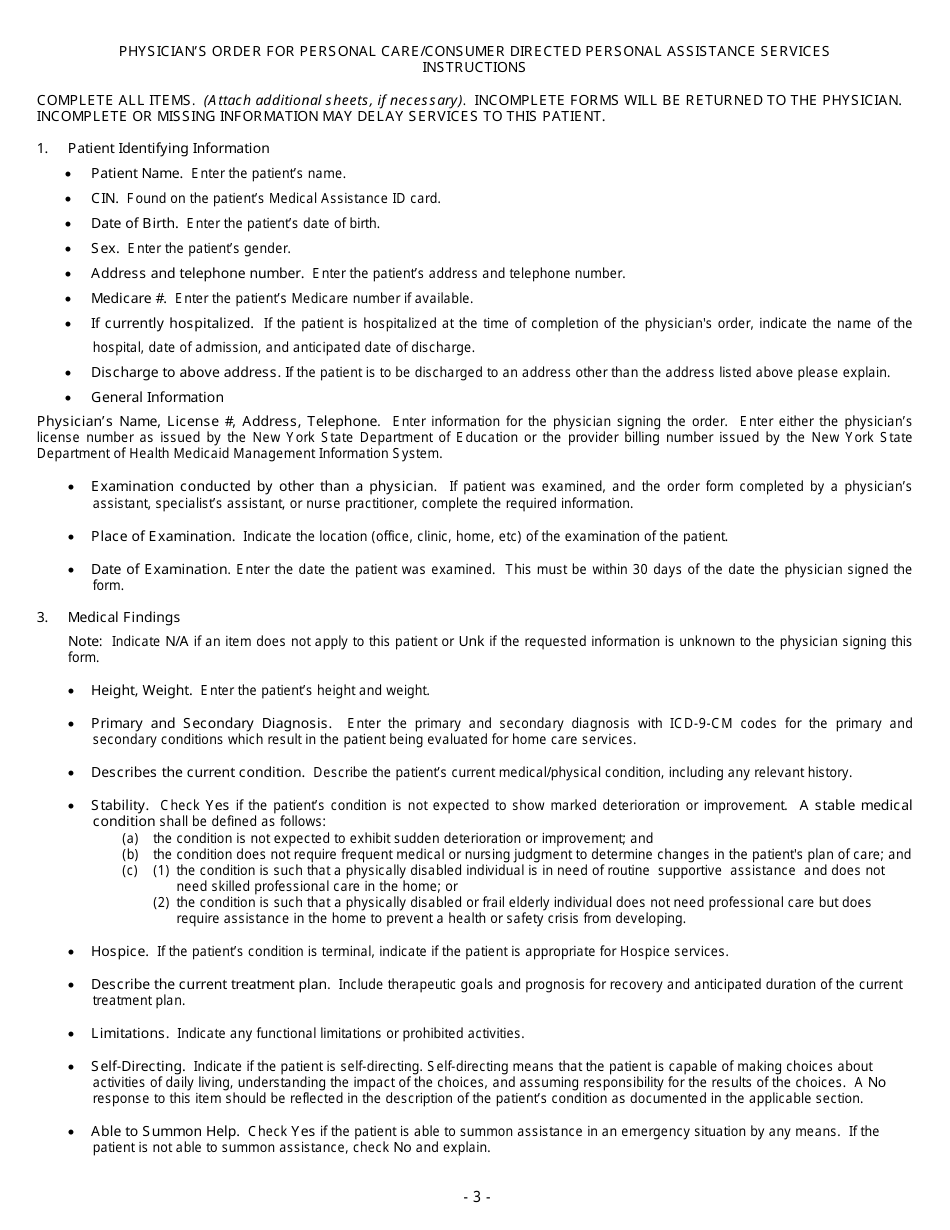
Form DOH-4359 Instructions
The document consists of several parts that are dedicated to different types of information the physician is supposed to collect. If they struggle with some of the sections, the order is followed by two pages of instructions. These guidelines provide information on how tofill out the DOH-4359 Form, as well as where and when to file it. The parts that must be completed include the following:
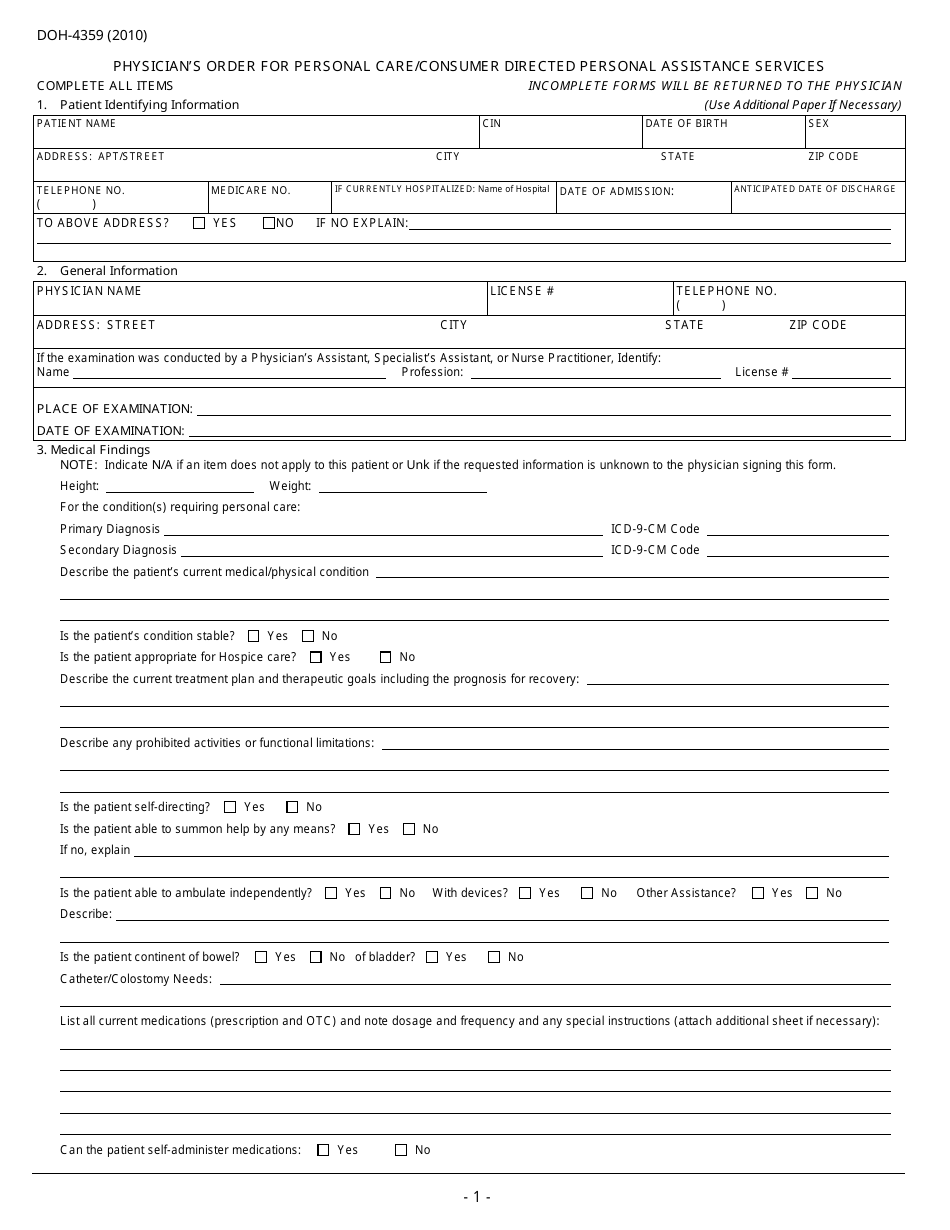
- Information About the Patient . In the first part of the document, the physician is required to provide information about their patient. It includes the name of the patient, their date of birth, gender, contact details, and Medicare number.
- Information About the Physician . Here the physician must designate their full name, license number, and contact details.
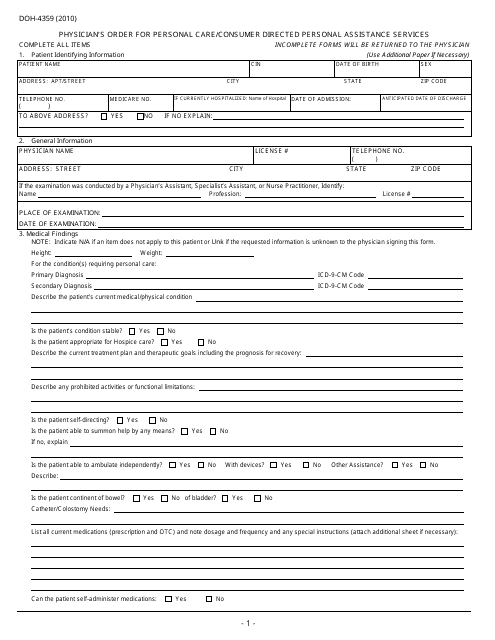
- Examination Details . Physicians must use this section of the form to state when and where they have performed the examination of their patients.
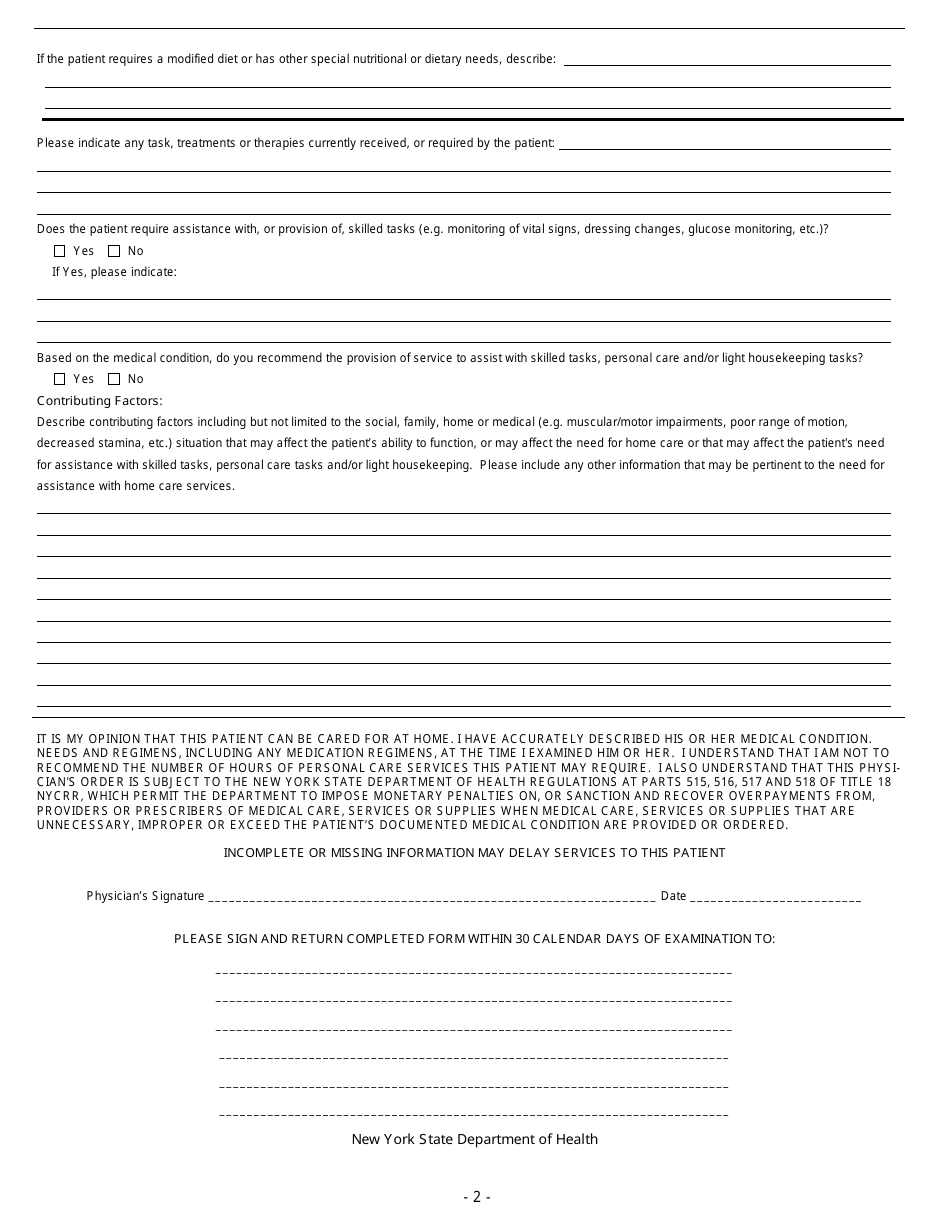
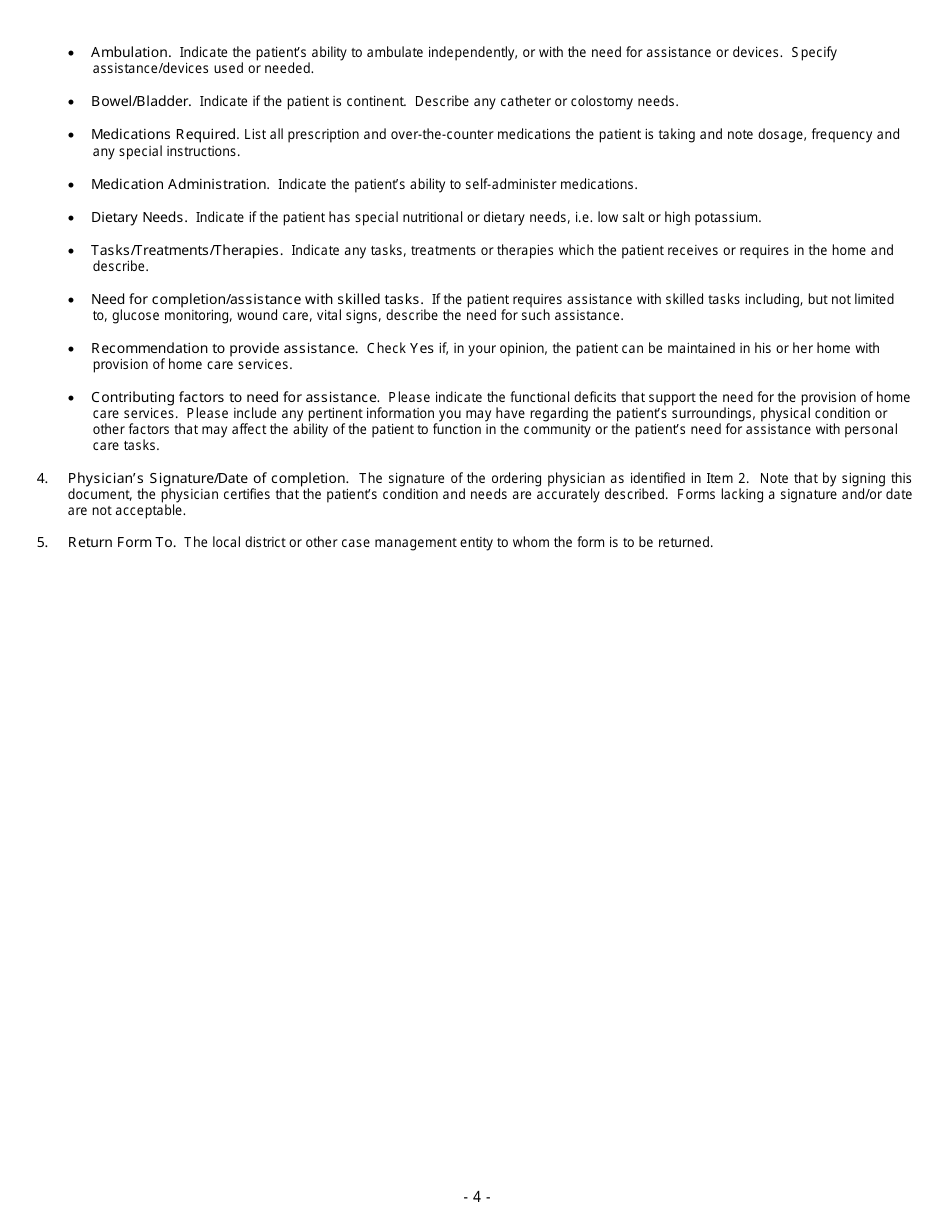
- Medical Findings . The physician is supposed to use this part of the document to indicate the patient's health information. It includes the patient's diagnosis, the description of their medical and physical condition, any limitations, activities that they are prohibited from performing, and other types of medical information.
- Signature and Date . At the end of the form, the physician must verify that the information they collected from the examination is correct. To validate it they must sign and date the document.
Download Form DOH-4359 Physician's Order for Personal Care / Consumer Directed Personal Assistance Services - New York
1
2

3

4