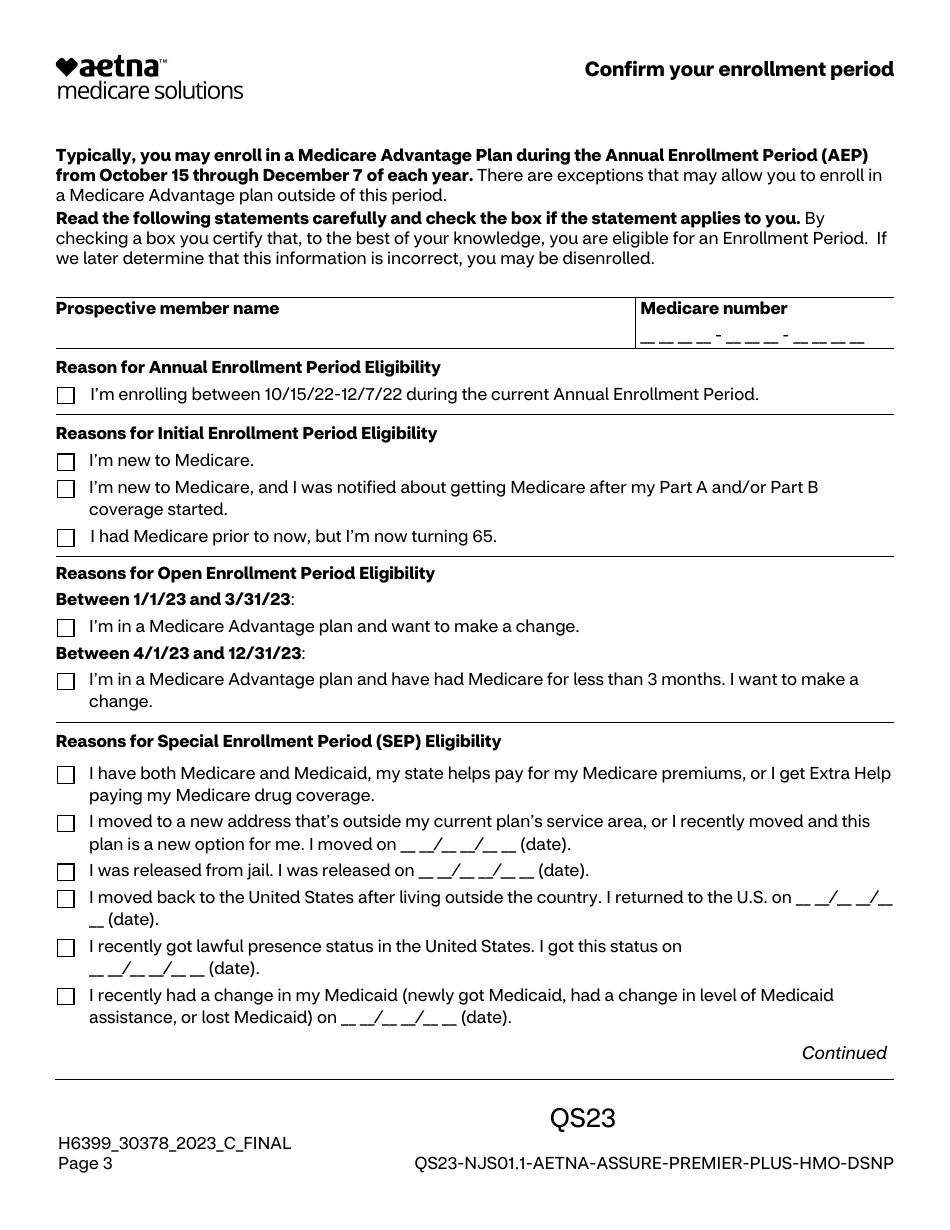
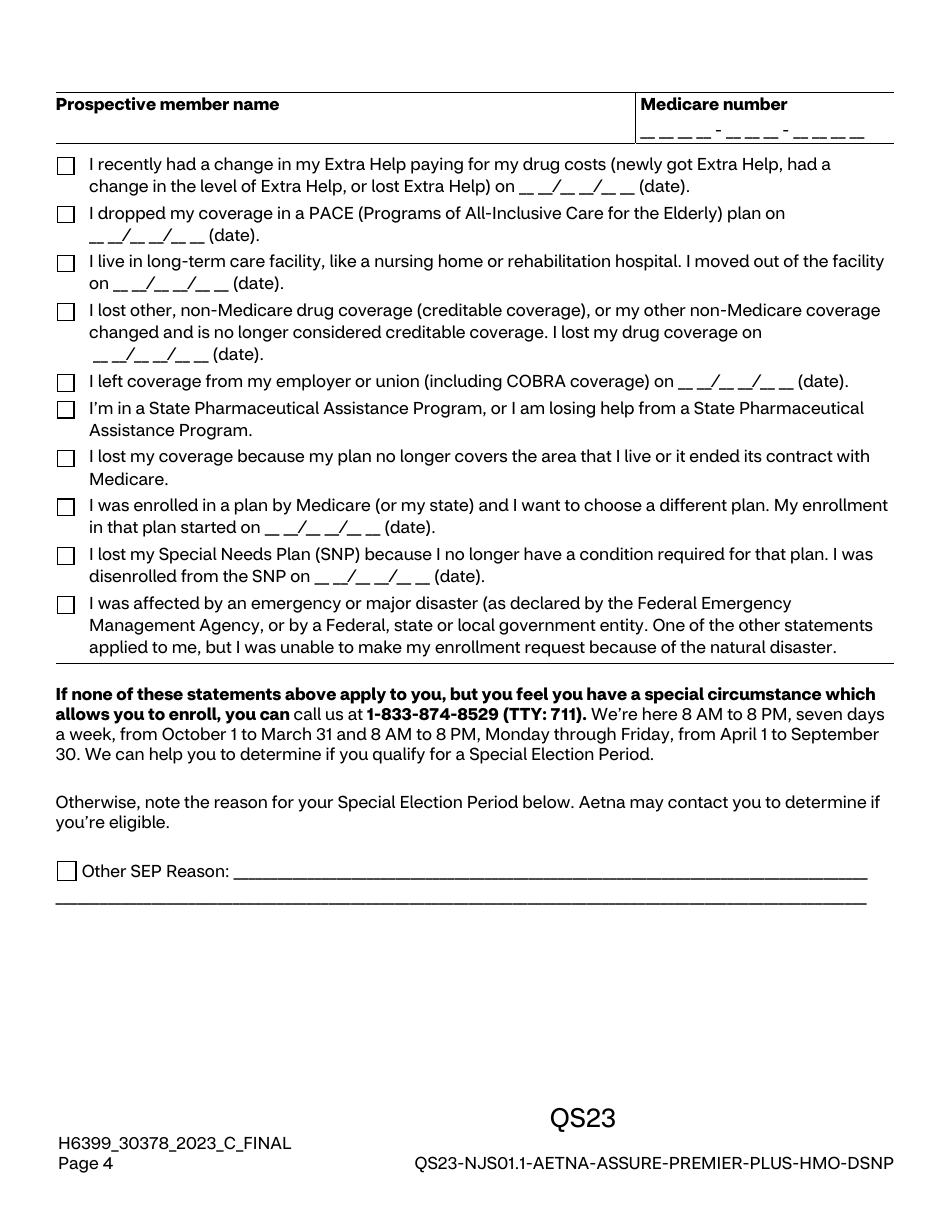
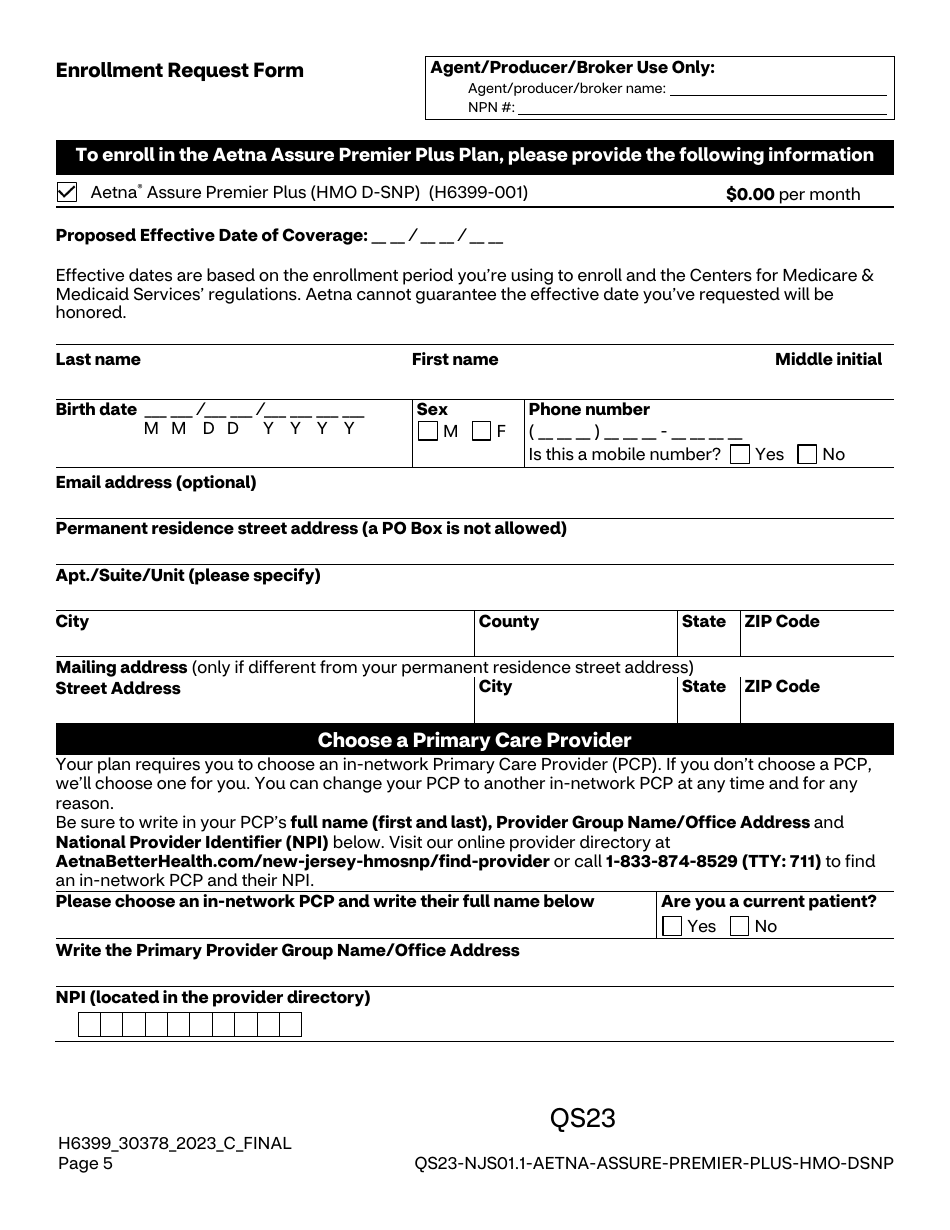
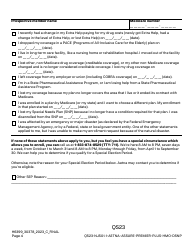
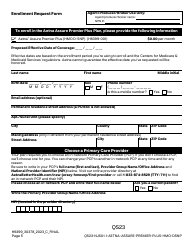
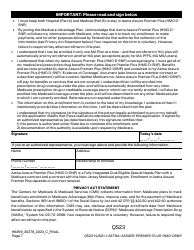
Aetna Assure Premier Plus Plan (HMO D-Snp) Individual Enrollment Request Form
The Aetna Assure Premier Plus Plan (HMO D-SNP) Individual Enrollment Request Form is used by individuals who want to enroll in this specific health insurance plan offered by Aetna. D-SNP stands for Dual Eligible Special Needs Plans, which are designed to provide care for people who qualify for both Medicare and Medicaid. The form captures important information from the enrollee needed to process their request for this plan, such as their personal details, contact information, Medicare and Medicaid eligibility details, and chosen primary care physician. This helps Aetna ensure that those applying meet all the necessary eligibility requirements. After completion, the form is submitted to Aetna for review.
The Aetna Assure Premier Plus Plan (HMO D-SNP) Individual Enrollment Request Form is filed by individuals who are eligible, and wish to enroll in the health care coverage provided by Aetna under this specific plan. These individuals typically have both Medicare and Medicaid and reside within the plan's specific service area. The form is used to gather necessary information and consent to begin coverage under this plan.
FAQ
Q: What is the Aetna Assure Premier Plus Plan (HMO D-Snp)?
A: Aetna Assure Premier Plus Plan is an all-in-one Medicare Advantage plan that provides coverage for medical, surgical, and pharmaceutical needs. The (HMO D-Snp) reference denotes it as a Health Maintenance Organization Dual Eligible Special Needs Plan, which means it is designed for beneficiaries who are eligible for both Medicare and Medicaid.
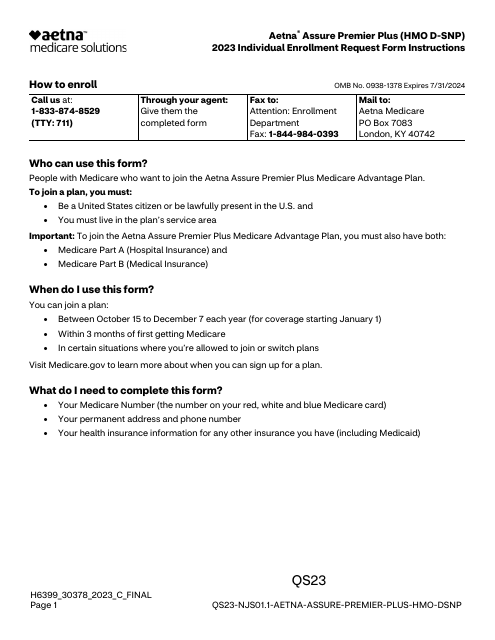
Q: How can one enroll in the Aetna Assure Premier Plus Plan (HMO D-Snp)?
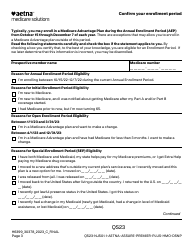
A: Individuals can enroll in the Aetna Assure Premier Plus Plan (HMO D-Snp) by filling out an Individual Enrollment Request Form. This form can be filled and submitted during the designated Medicare annual election or special election periods.
Q: Who is eligible for Aetna Assure Premier Plus Plan (HMO D-Snp)?
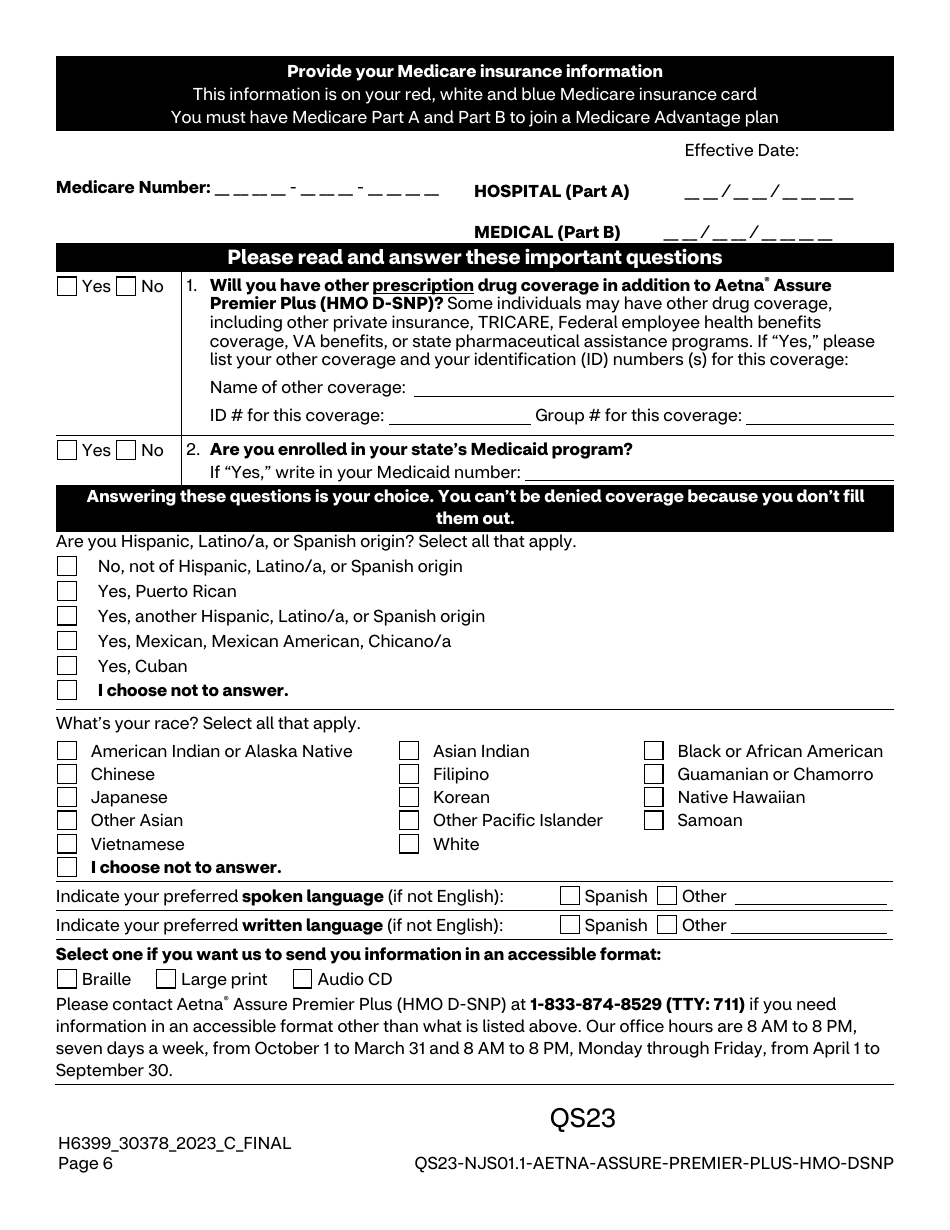
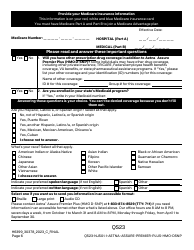
A: Eligibility for the Aetna Assure Premier Plus Plan (HMO D-Snp) is for individuals who are enrolled in both Medicare Part A and Part B, receive Medicaid benefits, and live within the plan's service area.
Q: Can any doctor be visited under the Aetna Assure Premier Plus Plan?
A: As an HMO plan, the Aetna Assure Premier Plus Plan typically requires you to see doctors within their network. Specialists' services may require referrals. It's always best to consult Aetna's list of network providers or contact their customer service for specific coverage details.
Q: Does the Aetna Assure Premier Plus Plan (HMO D-Snp) cover prescription drugs?
A: Yes, the Aetna Assure Premier Plus Plan (HMO D-Snp) includes coverage for prescription drugs, assisting beneficiaries with the cost of their necessary medications.
Download Aetna Assure Premier Plus Plan (HMO D-Snp) Individual Enrollment Request Form

1

2

3

4
5

6
7

8
9

10
11

12
13

14
15

16
17

18