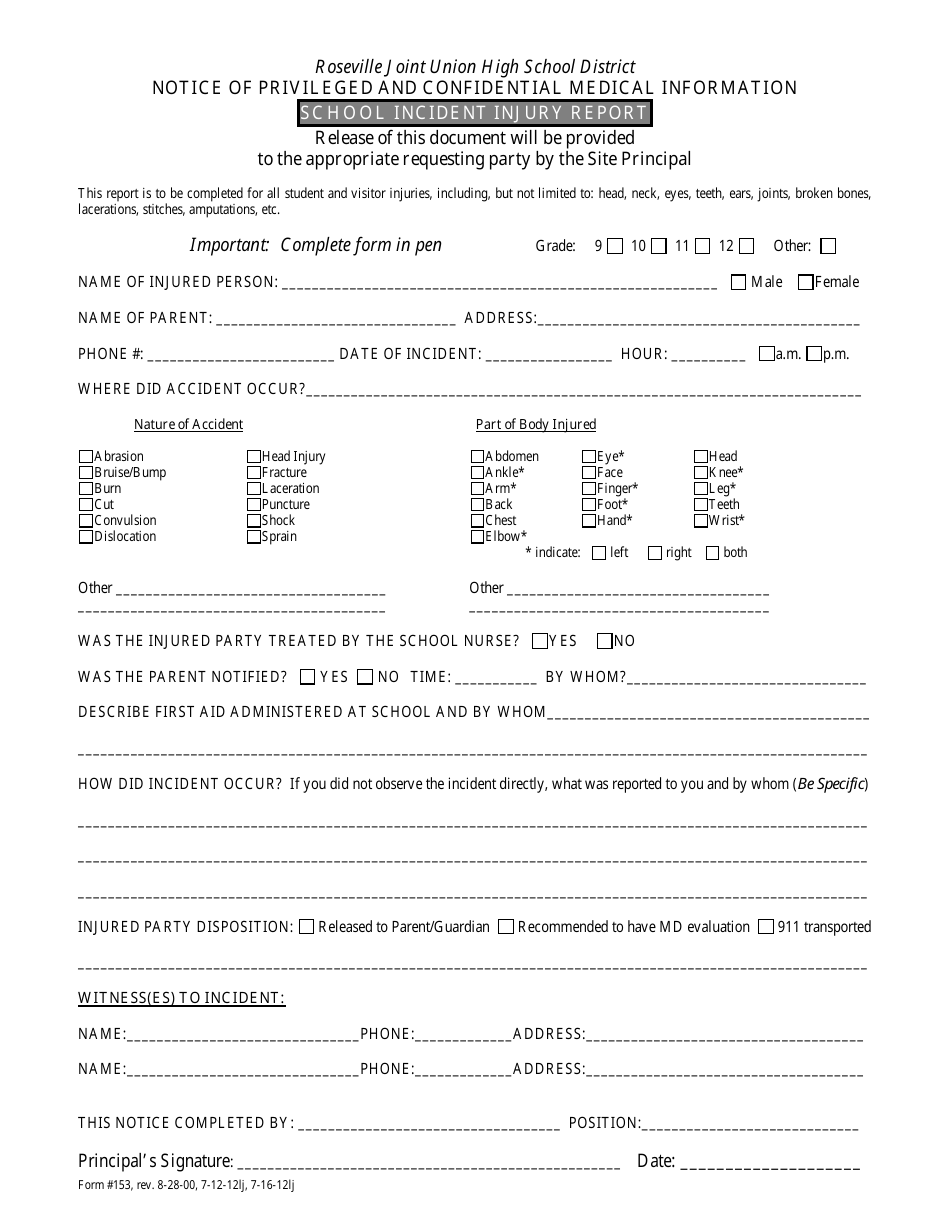
School Incident Injury Report Form - Roseville Joint Union High School District
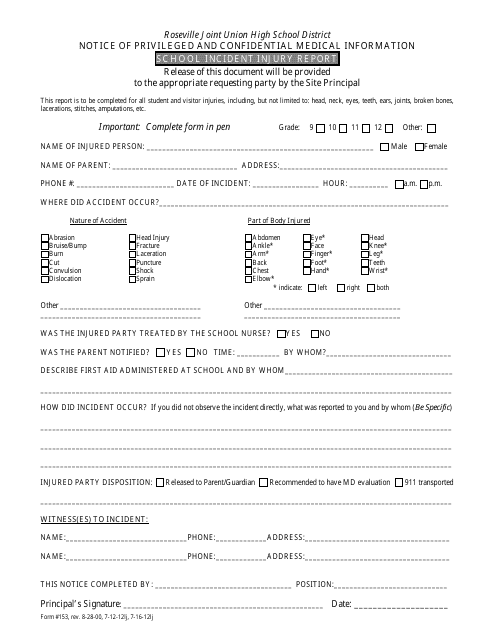
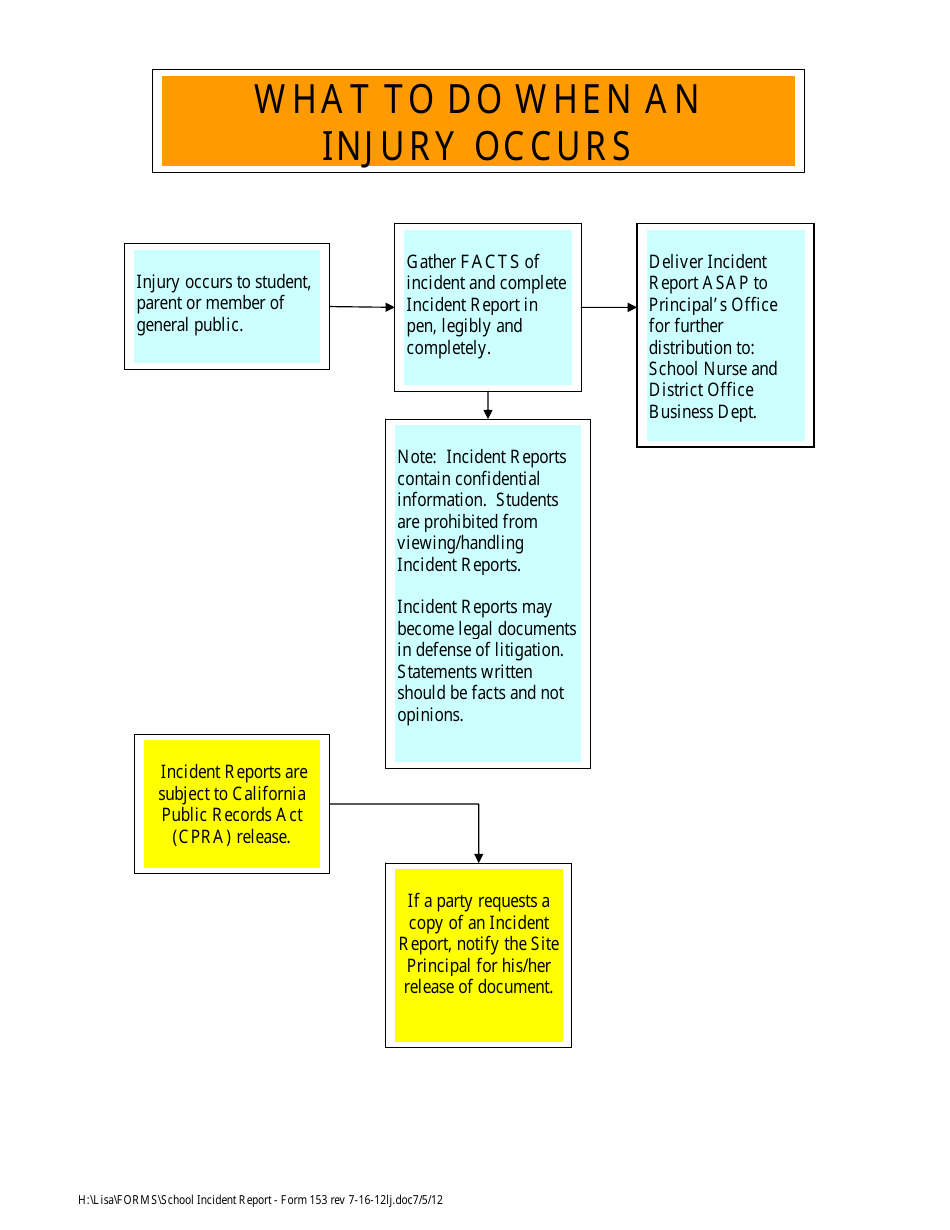
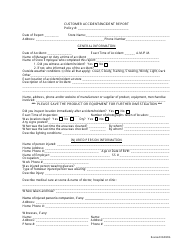
The School Incident Injury Report Form is used by the Roseville Joint Union High School District to report and document any injuries that occur on school premises or during school activities. This form helps in maintaining a record of incidents and assists in ensuring appropriate medical treatment and follow-up, as well as identifying any safety concerns that need to be addressed.
The school incident injury report form is typically filed by the school staff, such as teachers or administrators, at the Roseville Joint Union High School District.
FAQ
Q: What is the School Incident Injury Report Form?
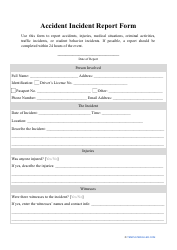
A: The School Incident Injury Report Form is a document used by Roseville Joint Union High School District to report and document any injuries or incidents that occur on school grounds.
Q: Why is the School Incident Injury Report Form important?
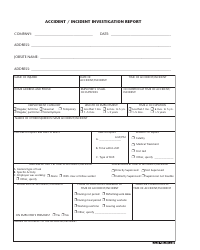
A: The form is important because it helps the school district keep track of any incidents or injuries that happen at school, ensuring that proper documentation and follow-up can be done if necessary.
Q: Who should fill out the School Incident Injury Report Form?
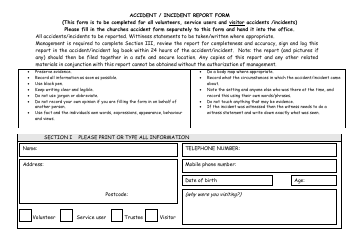
A: The form should be filled out by any staff member or witness who is involved in or observes an incident or injury at the school.
Q: What information is typically included in the School Incident Injury Report Form?
A: The form will usually ask for details about the incident, such as the date, time, location, description of the injury, and any witnesses or individuals involved.
Download School Incident Injury Report Form - Roseville Joint Union High School District

1

2