Ohio Department of Medicaid Forms
The Ohio Department of Medicaid is responsible for administering the Medicaid program in the state of Ohio. Medicaid is a joint federal and state program that provides healthcare coverage to eligible low-income individuals and families. The Ohio Department of Medicaid ensures that eligible Ohio residents have access to affordable healthcare services by managing the enrollment process, determining eligibility, and working with healthcare providers to coordinate care for Medicaid beneficiaries.
Documents:
205
This form is used for understanding your rights and responsibilities as a consumer of Medicaid health coverage in Ohio. It provides information about what you are entitled to as well as what is expected of you as a Medicaid recipient. This document helps you navigate your health coverage effectively.
This Form is used for requesting a hardship exemption in the state of Ohio.
This form is used for submitting a medical claim review request in Ohio.
This Form is used for adding an addendum to Form ODM03623 for Intermediate Care Facilities for the Mentally Retarded (ICFs/MR) in Ohio. It specifically addresses Behavioral Redirection and Medical Monitoring Outlier Services.
This Form is used for adding an additional note to the ODM03623 form specifically for Nursing Facilities (NFS) in Ohio providing Pediatric Outlier Services.
This form is used for nursing facilities in Ohio to request traumatic brain injury outlier services.
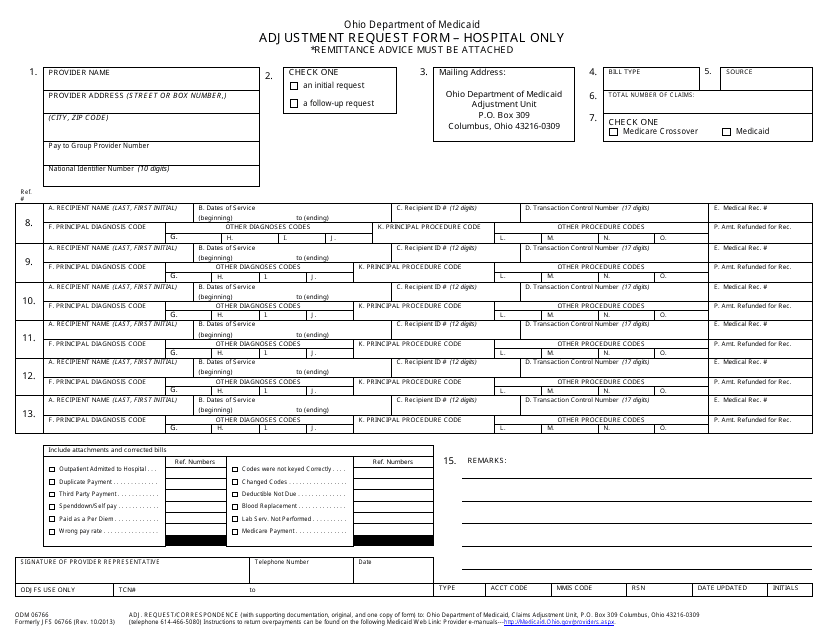
This form is used for submitting an adjustment request specifically for hospitals in the state of Ohio.
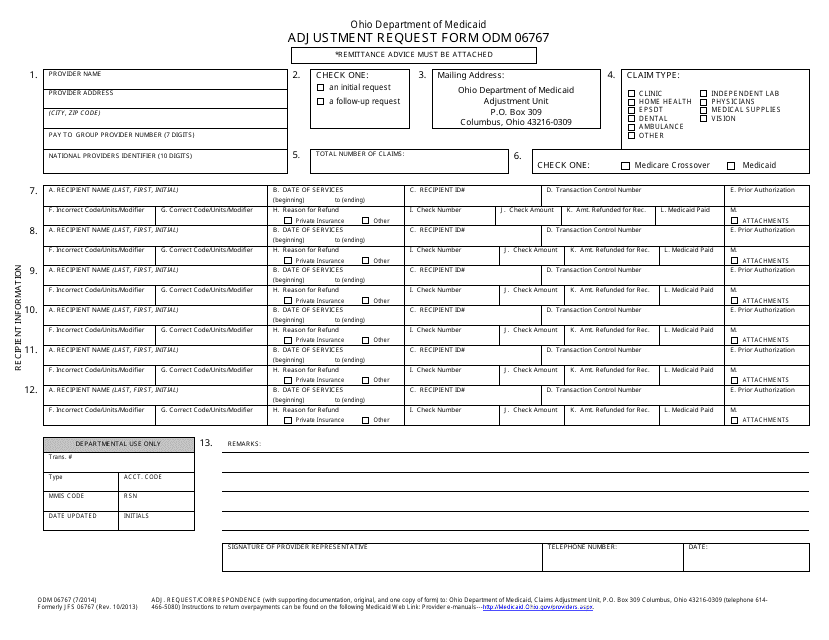
This form is used for submitting an adjustment request in the state of Ohio.
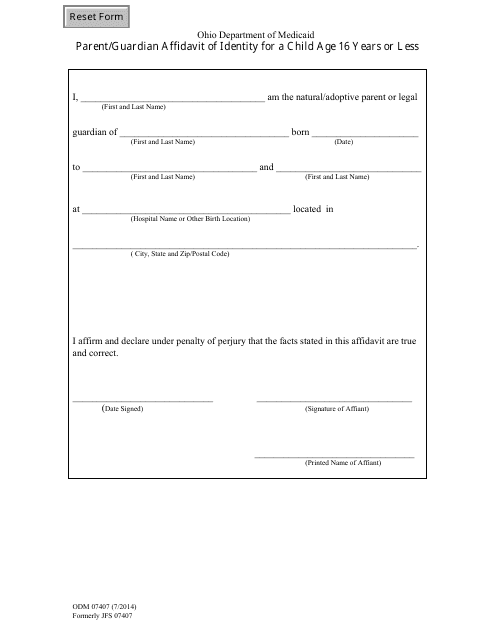
This form is used for parents or guardians in Ohio to provide an affidavit of identity for a child who is 16 years old or younger.
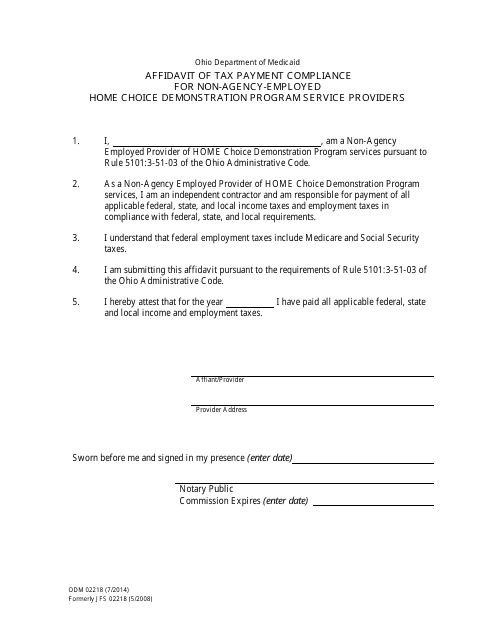
This document is used for non-agency-employed service providers participating in the Home Choice Demonstration Program in Ohio. It is an affidavit of tax payment compliance.
This form is used for authorizing an agreement between the state Medicaid program and an ICF-MR facility in Ohio for individual assessments.
This form is used for authorizing the issuance of a certificate of group health plan coverage in the state of Ohio.
This Form is used for declaring the coverage of a Group Health Plan in Ohio. It provides a certificate stating the details of the plan and the coverage it offers.
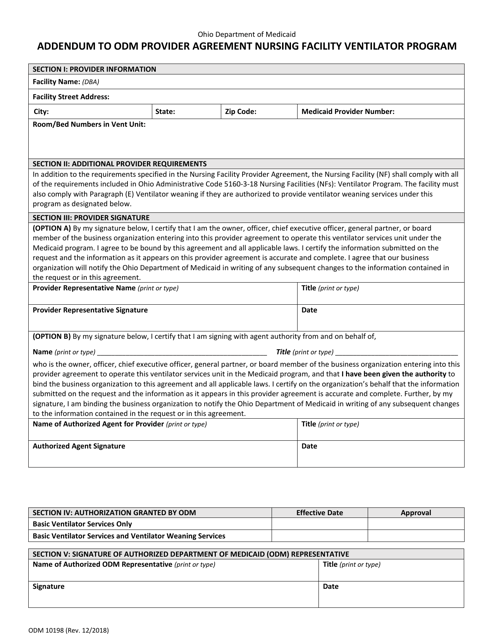
This document is an addendum to the ODM provider agreement for the Nursing Facility Ventilator Program in Ohio. It includes additional information and terms related to the program.
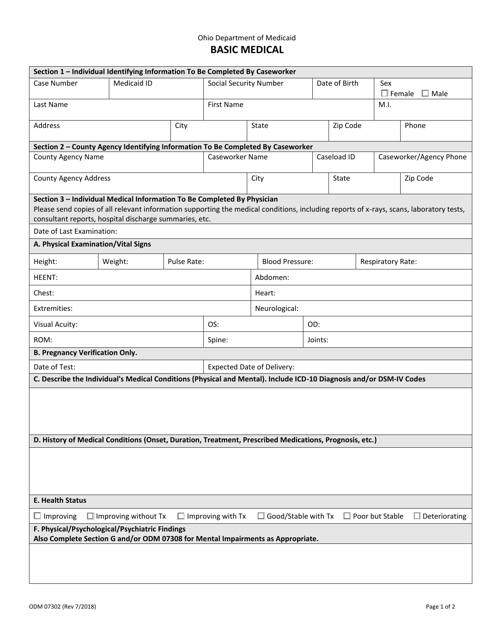
This Form is used for basic medical purposes in the state of Ohio.
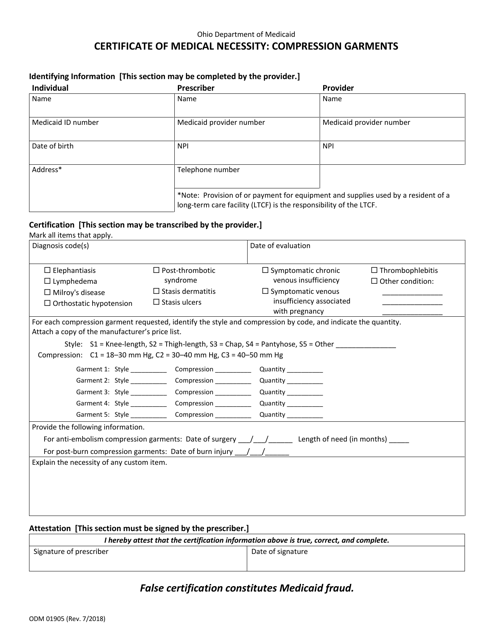
This form is used for requesting a certificate of medical necessity for compression garments in the state of Ohio.
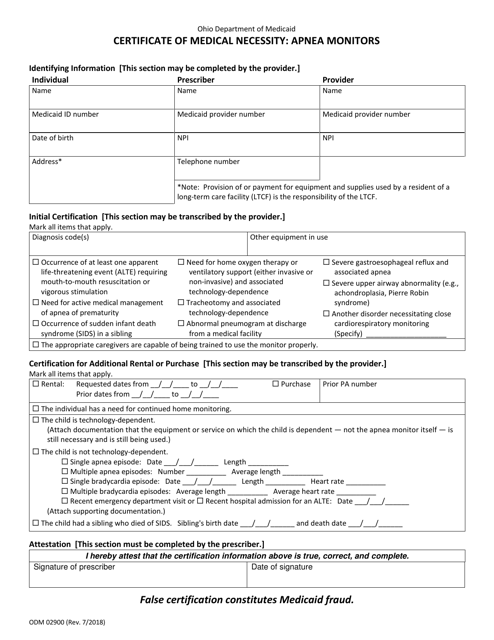
This form is used for obtaining a Certificate of Medical Necessity for Apnea Monitors in the state of Ohio. It is required for individuals who need these monitors for medical reasons.
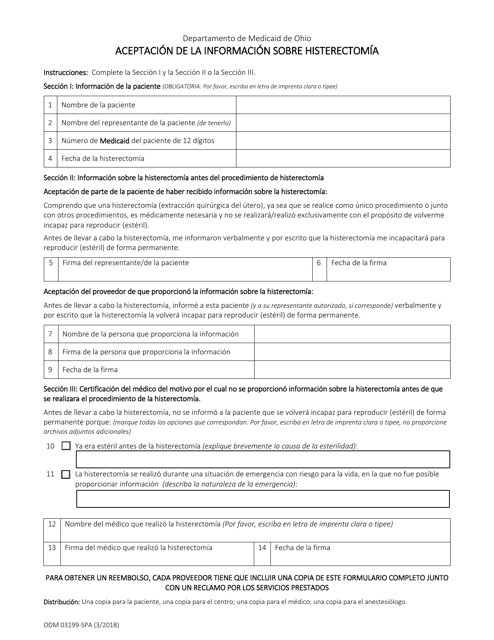
This type of document is used for accepting information about a hysterectomy in Ohio, and it is in Spanish.
This Form is used for Spanish-speaking parents or legal guardians in Ohio to make a sworn statement about the identity of a child under the age of 16.
This Form is used for making a sworn statement by third parties regarding place of birth or nationality in Ohio. It is written in Spanish.
This type of document, Formulario ODM06723-SPA Designacion De Representante Autorizado - Ohio (Spanish), is used for designating an authorized representative in Ohio.
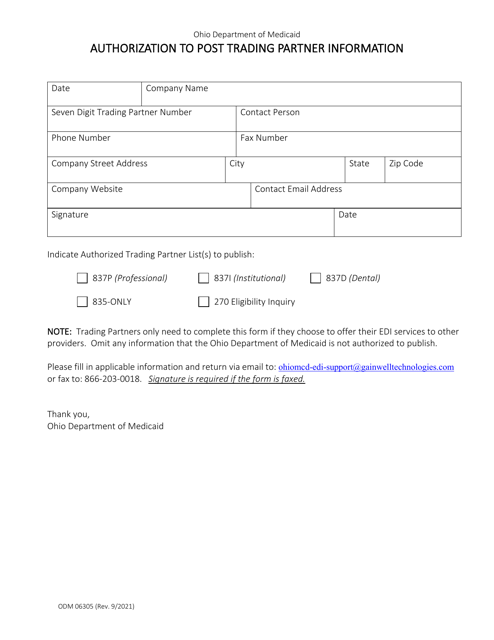
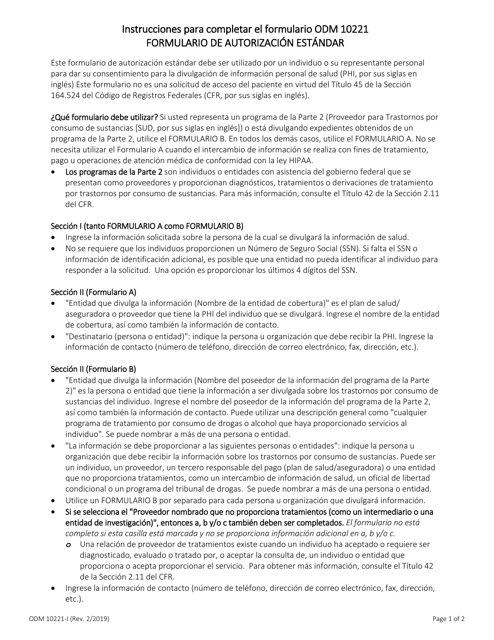
This type of document is a standard authorization form in Ohio, written in Spanish.
Este formulario se utiliza para solicitar servicios basados en el hogar y la comunidad en Ohio.