Ohio Department of Medicaid Forms
Documents:
205
This document is for certifying Ohio Medicaid Managed Care encounter data. It is used to ensure accuracy and compliance with Ohio Medicaid guidelines.
This form is used to designate an authorized representative for home care attendant services in Ohio.
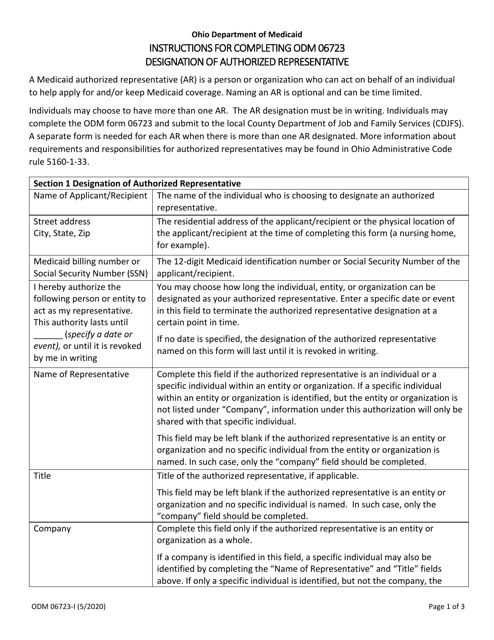
This Form is used for designating an authorized representative in the state of Ohio.
This Form is used for communication between facilities in the state of Ohio.
This form is used for requesting health insurance information in the state of Ohio.
This form is used for creating a Health and Safety Action Plan specific to the state of Ohio.
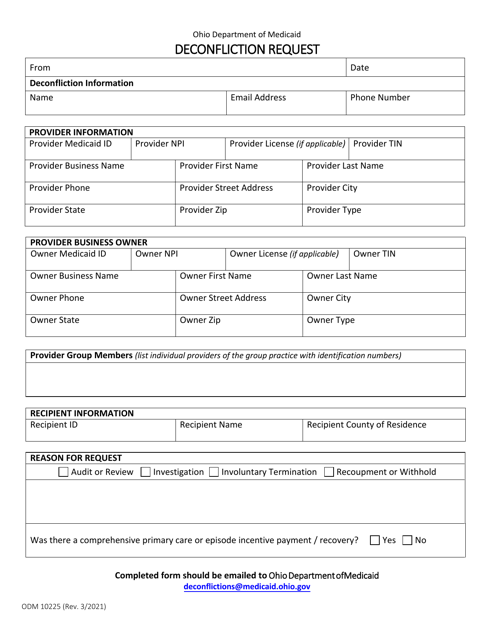
This form is used for submitting a deconfliction request in the state of Ohio. Deconfliction is a process that helps ensure the coordination and safety of activities involving multiple agencies or organizations. The form is used to request clearance and coordinate activities to prevent conflicts or overlapping events.
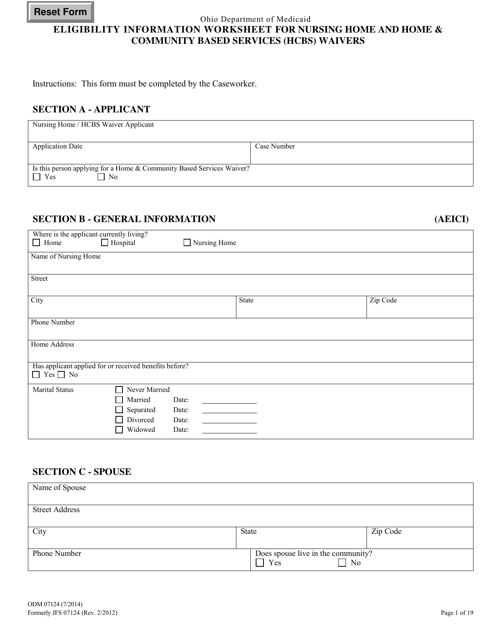
This form is used for gathering eligibility information for individuals seeking nursing home and Home & Community Based Services (HCBS) waivers in the state of Ohio.
This Form is used for updating personal information in Ohio.
This document is used for verifying the settings of Home and Community-Based Services (HCBS) in Ohio.
This Form is used for requesting a Mac computer in the state of Ohio.
This form is used for requesting participation in the Managed Care & Mycare Ohio Organization Pilot Program in Ohio.
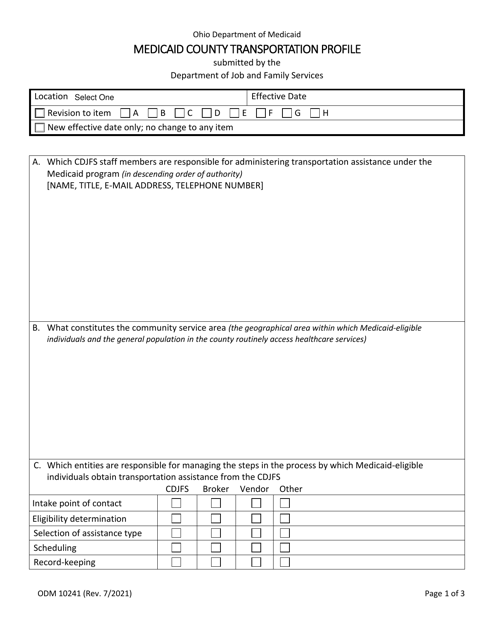
This form is used for Medicaid County Transportation Profile in the state of Ohio.

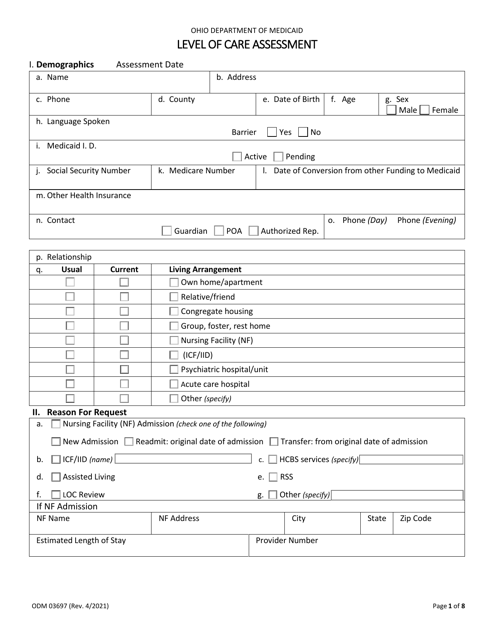
This Form is used for conducting a Level of Care Assessment in Ohio. It helps determine the appropriate level of care for an individual in need of long-term care services.
This form is used for reporting cases of Medicaid fraud in the state of Ohio.
This Form is used for calculating budget and resources for Medicaid in Ohio for non-institutional care.
This Form is used for requesting an interim payment from Medicaid for healthcare providers in Ohio.
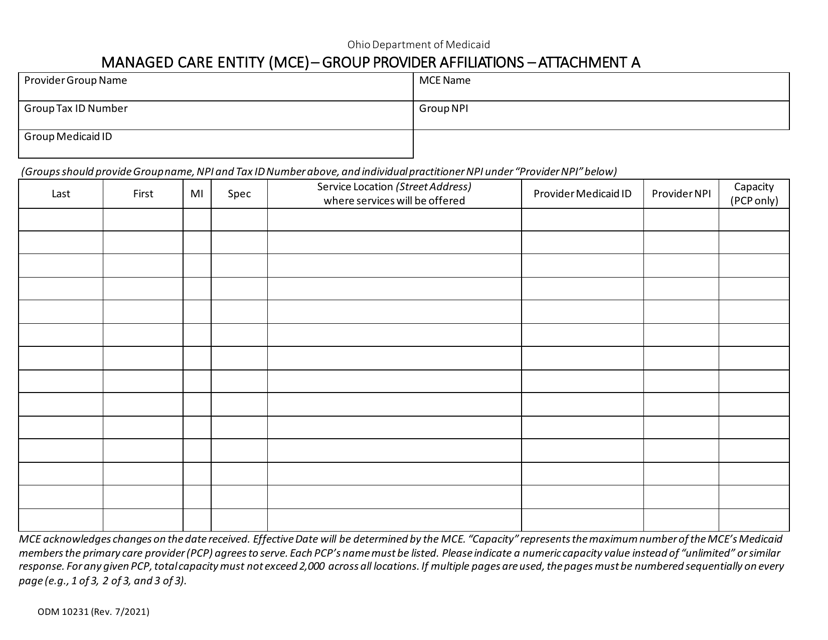
This form is used for reporting non-primary providers in the state of Ohio for the Mcp program.
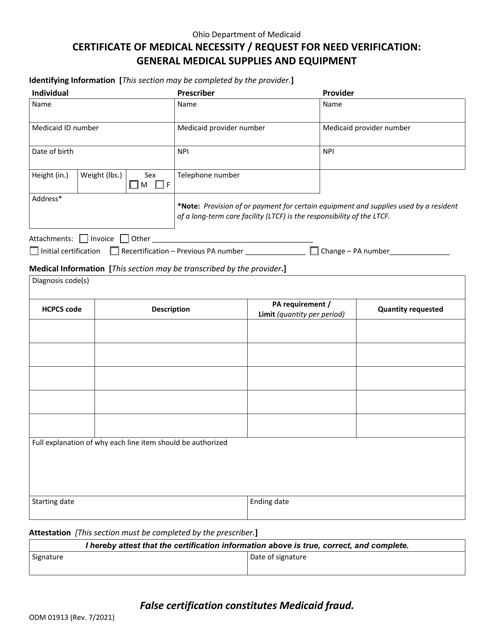
This form is used for obtaining a certificate of medical necessity for wheelchairs in the state of Ohio.
This Form is used for conducting a mental functional capacity assessment in the state of Ohio. It is used to evaluate an individual's cognitive and emotional abilities to determine their overall mental functioning.
This document is used to notify individuals in Ohio when their managed care plan denies medical services. It informs them of the reasons for the denial and provides instructions for appealing the decision.
This Form is used for reporting Medicaid Quality Control (MEQC) case findings in Ohio.
This form is used for hospital services in Ohio. It is an attachment to Form ODM10233.
This Form is used for informing individuals in Ohio about the denial of payment for medical services by their managed care plan.
This form is used for notifying Medicaid Estate Recovery about a pending transfer of property through a Transfer on Death Deed in Ohio.
This Form is used for notifying individuals about Medicaid overpayments in the state of Ohio. It provides information about the amount owed and instructions for repayment.
This Form is used for healthcare providers in Ohio to create a treatment plan for their patients.
This form is used for verifying a Qualified Income Trust in Ohio. It is required for individuals who need to qualify for Medicaid long-term care benefits and have income above the threshold.
This form is used for obtaining a Certificate of Medical Necessity for incontinence items in the state of Ohio.
This Form is used for long-term care facilities in Ohio to enter into a Medicaid provider agreement with the state.
