Ohio Department of Medicaid Forms
Documents:
205
This form is used for healthcare providers in Ohio to apply for a Medicaid provider number specifically for managed care plans.
This form is used to notify individuals in Ohio about their personal needs allowance (PNA) account remittance. It provides information about the funds being deposited into their account for personal expenses.
This form is used for reporting the quarterly ventilator program data for nursing facilities in Ohio. It is used to track and monitor the usage of ventilators in these facilities.
This Form is used for notifying pregnant women in Ohio about potential risks during prenatal care.
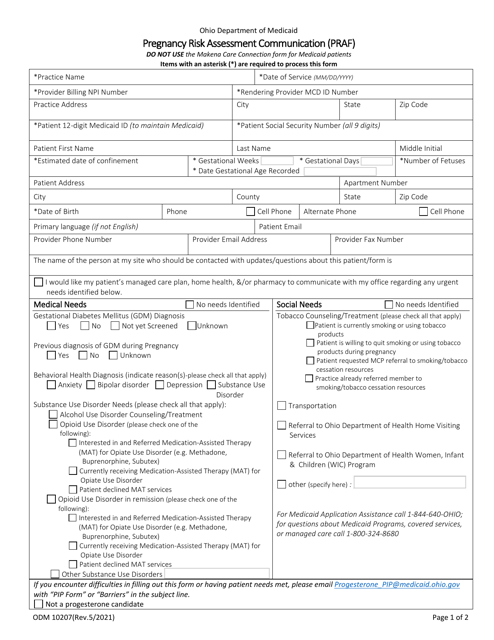
This Form is used for communicating pregnancy risk assessment in Ohio.
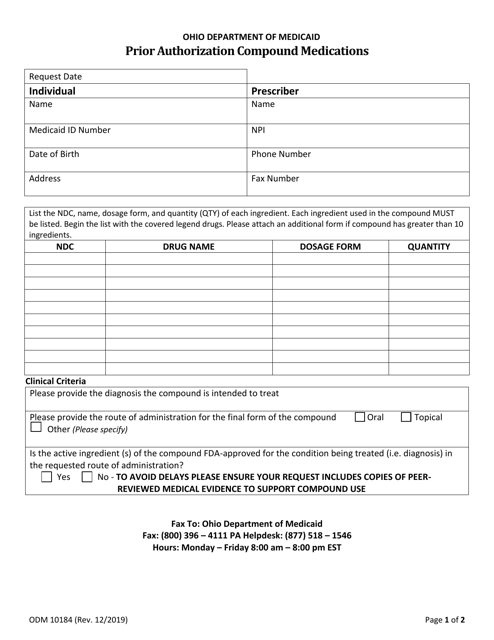
This form is used for obtaining prior authorization for compound medications in the state of Ohio. It is necessary to submit this form in order to receive coverage for the cost of these medications.
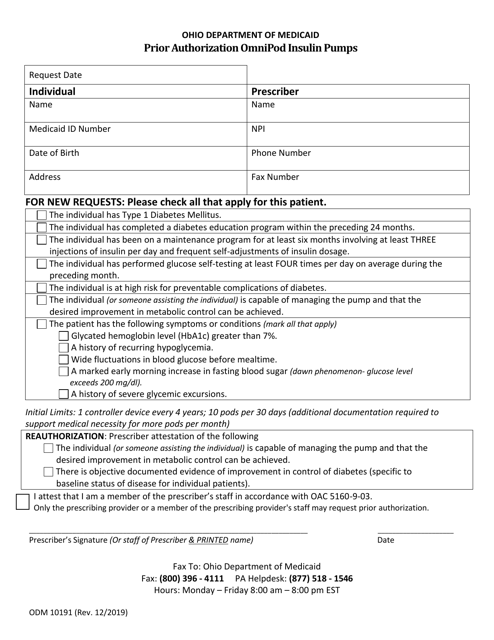
This Form is used for requesting prior authorization for Omnipod insulin pumps in the state of Ohio.
This form is used for obtaining prior authorization for the medication Sublocade in the state of Ohio. It is required for patients to access this specific medication.
This Form is used for obtaining certification for abortion in the state of Ohio. It is a required document for medical professionals performing abortions.
This form is used for notifying individuals in Ohio that they have failed to submit the necessary resource documentation for a resource assessment.
This Form is used for obtaining prior authorization for Synagis medication in the state of Ohio.
This form is used for obtaining prior authorization for oral medication-assisted treatment of opioid use disorder in the state of Ohio. It is required for patients seeking this type of treatment.
Form ODM10229 Certificate of Medical Necessity: High-Frequency Chest Wall Oscillation Devices - Ohio
This Form is used for obtaining a Certificate of Medical Necessity for High-Frequency Chest Wall Oscillation Devices in Ohio.
This form is used for assessing the outcome of private duty nursing (PDN) services in Ohio.
This form is used for referring individuals to the Program of All-inclusive Care for the Elderly (PACE) in Ohio.
This Form is used for notifying individuals in Ohio when their managed care plan is reducing, suspending, or terminating medical services. It ensures that individuals are informed of any changes to their healthcare coverage.
This form is used for Ohio managed care plan providers to apply for a provider reporting number.
This form is used for providing health insurance information in the state of Ohio.
This form is used for Medicaid providers in Ohio to submit their final settlement.
This form is used for requesting approval of claim specialty care transport (SCT) and related mileage in the state of Ohio.
This form is used for requesting a template for contract resources in Ohio.
This form is used for notifying Ohio authorities about a third party request for release related to a tort case.
This form is used for requesting verification of the need for repair of durable medical equipment, prostheses, or orthotic devices in Ohio.
This Form is used for requesting prior authorization for short-acting or long-acting opioid medication in Ohio.
This form is used for requesting prior authorization for prescription medications in the state of Ohio.
This form is used for requesting participation in the Ohio Death with Dignity Nursing Facility Ventilator Program.
This form is used for referring individuals to enroll in the Residential State Supplement (RSS) program in Ohio.
This Form is used for Medicaid providers in Ohio to submit their final settlement information.
This form is used for reporting the social summary for disability determination in the state of Ohio. It provides important information about an individual's social background and circumstances that may affect their eligibility for disability benefits.
This Form is used for evaluating referrals for comprehensive orthodontic treatment in Ohio.
This form is used for individuals in Ohio to provide a sworn statement confirming their birthplace or nationality, with the assistance of a third party.
This Form is used for requesting an exemption from step therapy in Ohio. Step therapy is a process where insurance companies require patients to try less expensive medications before covering more expensive ones. With this form, patients can request an exemption from this requirement.
This form is used for applying to participate in the Pharmacy Industry Day event in Ohio.
This form is used for providing a summary statement regarding a tort case in the state of Ohio.
This form is used for reporting the services provided in the state of Ohio.
This form is used for requesting a waiver for community transition services authorization in Ohio.
