![]() This version of the form is not currently in use and is provided for reference only. Download this version of
IRS Form 1095-B
for the current year.
This version of the form is not currently in use and is provided for reference only. Download this version of
IRS Form 1095-B
for the current year.
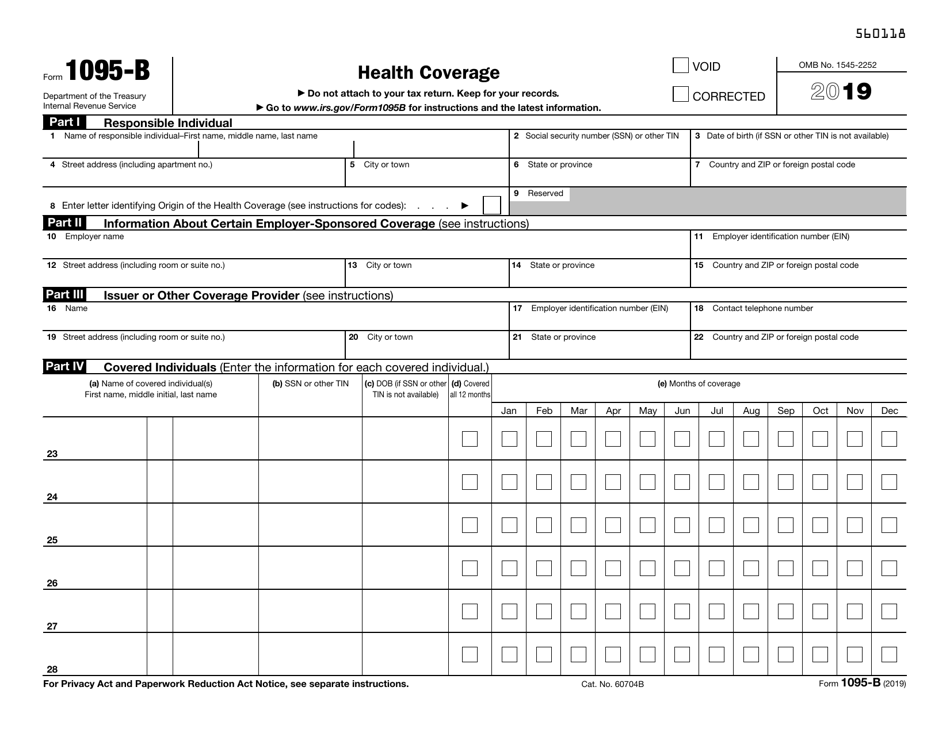
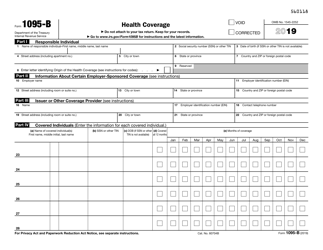
IRS Form 1095-B Health Coverage
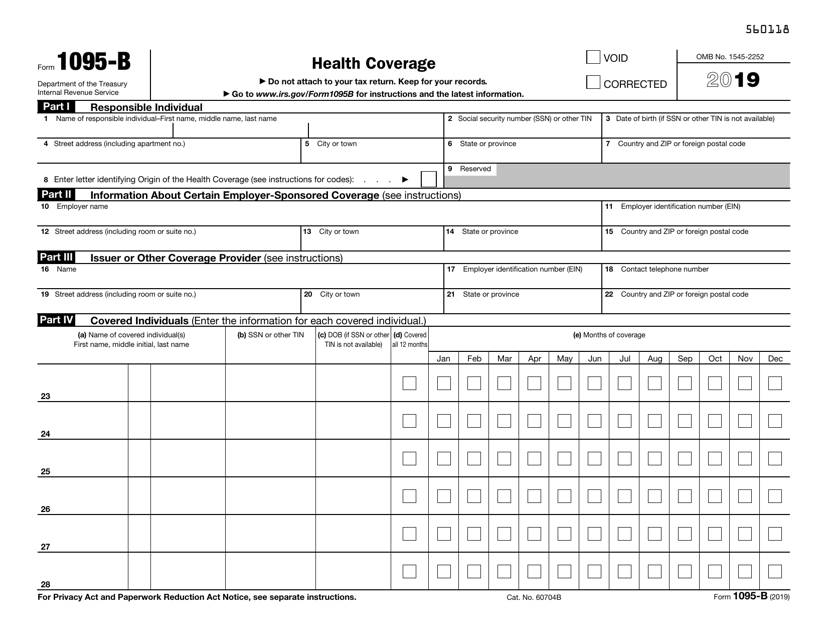

What Is Form 1095-B?
IRS Form 1095-B, Health Coverage , is a document used to submit certain information to the Internal Revenue Service (IRS) and to taxpayers about individuals who have minimum essential coverage and are not liable for the individual shared responsibility payment. Minimum essential coverage means individual market plans, plans sponsored by eligible employers, and programs sponsored by the government.
Alternate Name:
- IRS Health Coverage Form.
The latest version of the form was released by the IRS in 2019 with all previous editions obsolete. A fillable 1095-B form is available for download below. The Form 1095-B due date is the last day of February if you file it on paper and the last day of March if you file it electronically the year that follows the calendar year of coverage.
What Is 1095-B Form Used For?
The 1095-B Tax Form is a health insurance statement that reports the type of health care coverage you have, the dependents covered by your insurance policy, and the period of coverage for the previous calendar year. It verifies that you and your dependents have minimum qualifying health insurance coverage. Having an IRS 1095-B Form in hand is proof that you have the coverage required by the Affordable Care Act.
What Is the Difference Between 1095-B and 1095-C?
Sometimes people who are covered by insurance from their employer receive a copy of a related form, which is very similar to 1095-B - 1095-C, Employer-Provided Health Insurance Offer and Coverage. It contains substantially the same information, but it is generated by employers with 50 or more full-time employees. It is possible that some taxpayers receive both tax forms, which depends on how the employers' coverage is set up.
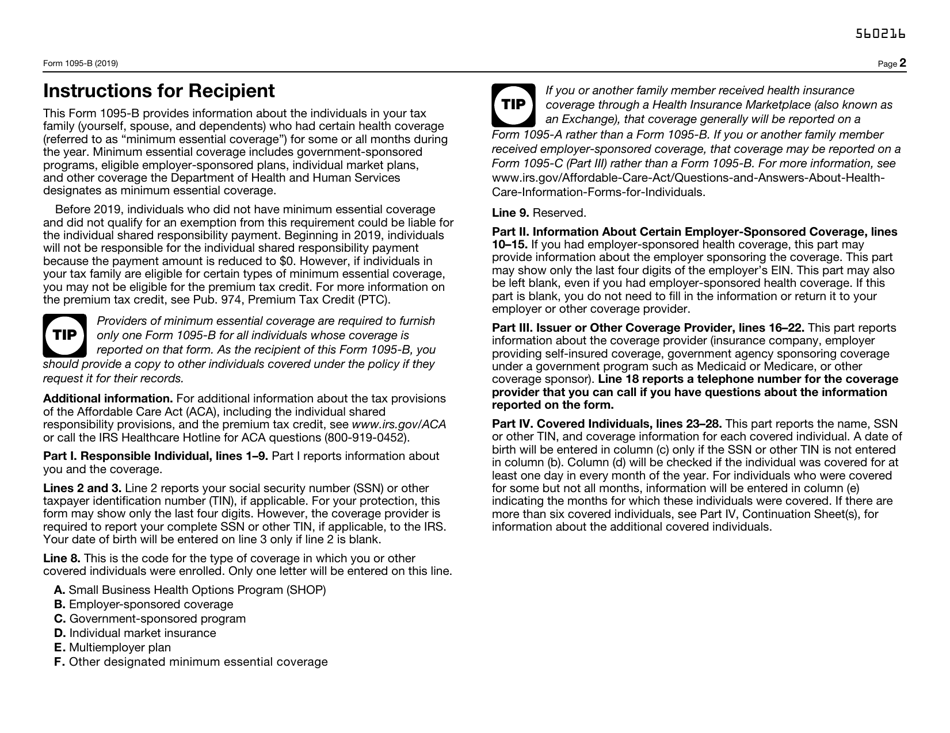
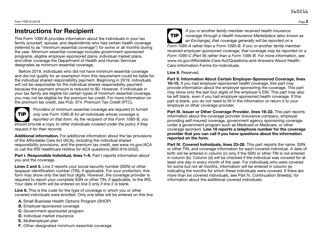
IRS Form 1095-B Instructions
-
You can send the form in a flat mailing. Do not paperclip or staple the forms together. You may send it in a package; however, bear in mind, that the IRS recommends filing the form electronically;
-
The mailing addresses for the form are:
- Department of the Treasury Internal Revenue Service Center Austin, TX 73301. Use this address for Alabama, Arizona, Arkansas, Connecticut, Delaware, Florida, Georgia, Kentucky, Louisiana, Maine, Massachusetts, Mississippi, New Hampshire, New Jersey, New Mexico, New York, North Carolina, Ohio, Pennsylvania, Rhode Island, Texas, Vermont, Virginia, West Virginia, and foreign countries;
- Department of the Treasury Internal Revenue Service Center PO Box 219256 Kansas City, MO 64121-9256. Use this address for Alaska, California, Colorado, District of Columbia, Hawaii, Idaho, Illinois, Indiana, Iowa, Kansas, Maryland, Michigan, Minnesota, Missouri, Montana, Nebraska, Nevada, North Dakota, Oklahoma, Oregon, South Carolina, South Dakota, Tennessee, Utah, Washington, Wisconsin, Wyoming;
-
There is a penalty of $270 for failure to submit a correct information return;
-
Check out the IRS-provided instructions for more information on filing and submitting the form.
How to Fill Out Form 1095-B?
- Part I, Responsible Individual. Provide information about the primary policyholder - the person who should receive the statement. Usually, it is a tax filer liable for the individual shared responsibility payment for the individuals covered. State this person's full name, social security number or date of birth, complete mailing address, and identify the origin of the health coverage. Consult with the separate instructions provided by the IRS to find out the responsible individual.
- Part II, Information About Certain Employer-Sponsored Coverage. Enter the name, employer identification number (EIN), and the complete mailing address of the employer who sponsors the coverage.
- Part III, Issuer or Other Coverage Provider. Enter the name, EIN, the complete mailing address, and the phone number of the coverage provider. It may be the carrier or issuer of insured coverage, the government agency that provided coverage, or a sponsor of a self-insured employer plan.
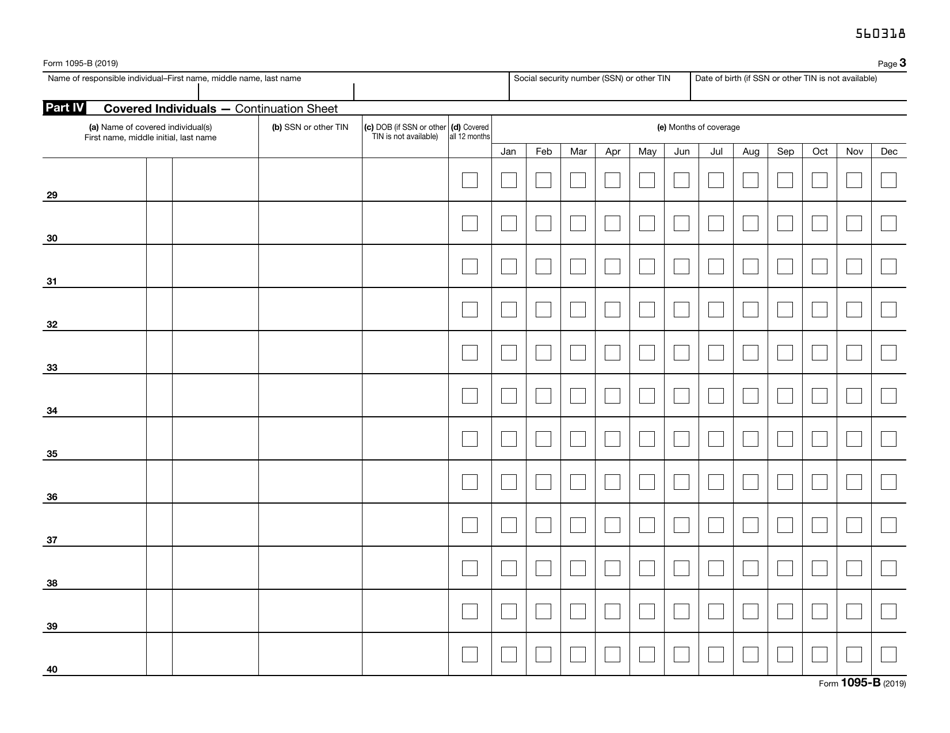
- Part IV, Covered Individuals. Provide the information on each individual covered - the full name, the social security number or the date of birth. State if the individual was covered for at least one day per month for all 12 months of the year. If not, check the boxes for the months in which the individual was covered. You can use the continuation sheet if there are more than six covered individuals.
IRS 1095-B Related Forms:
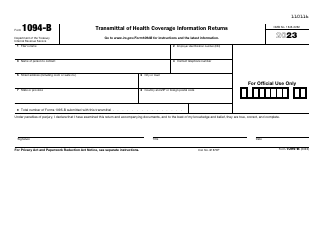
- IRS Form 1094-B, Transmittal of Health Coverage Information Returns, is a form used by the IRS to obtain information about individuals that have health coverage meeting the standards of the Affordable Care Act;
- IRS Form 1095-A, Health Insurance Marketplace Statement, is the main document in IRS Form 1095 Series and it is used to notify the IRS about the individuals that benefit from a qualified health plan acquired through the Health Insurance Marketplace. The health marketplace tax form is required to help people reconcile the credit on their returns with advance credit payments, to aid them in claiming the premium tax credit, and to complete a tax return without mistakes.
- IRS Form 1095-C, Employer-Provided Health Insurance Offer and Coverage, is a related form for the employers with 50 or more full-time employees that have to report to the IRS the information about health coverage and offers of health coverage required under sections 6055 and 6056 of the Internal Revenue Code.
Download IRS Form 1095-B Health Coverage
1
2
3