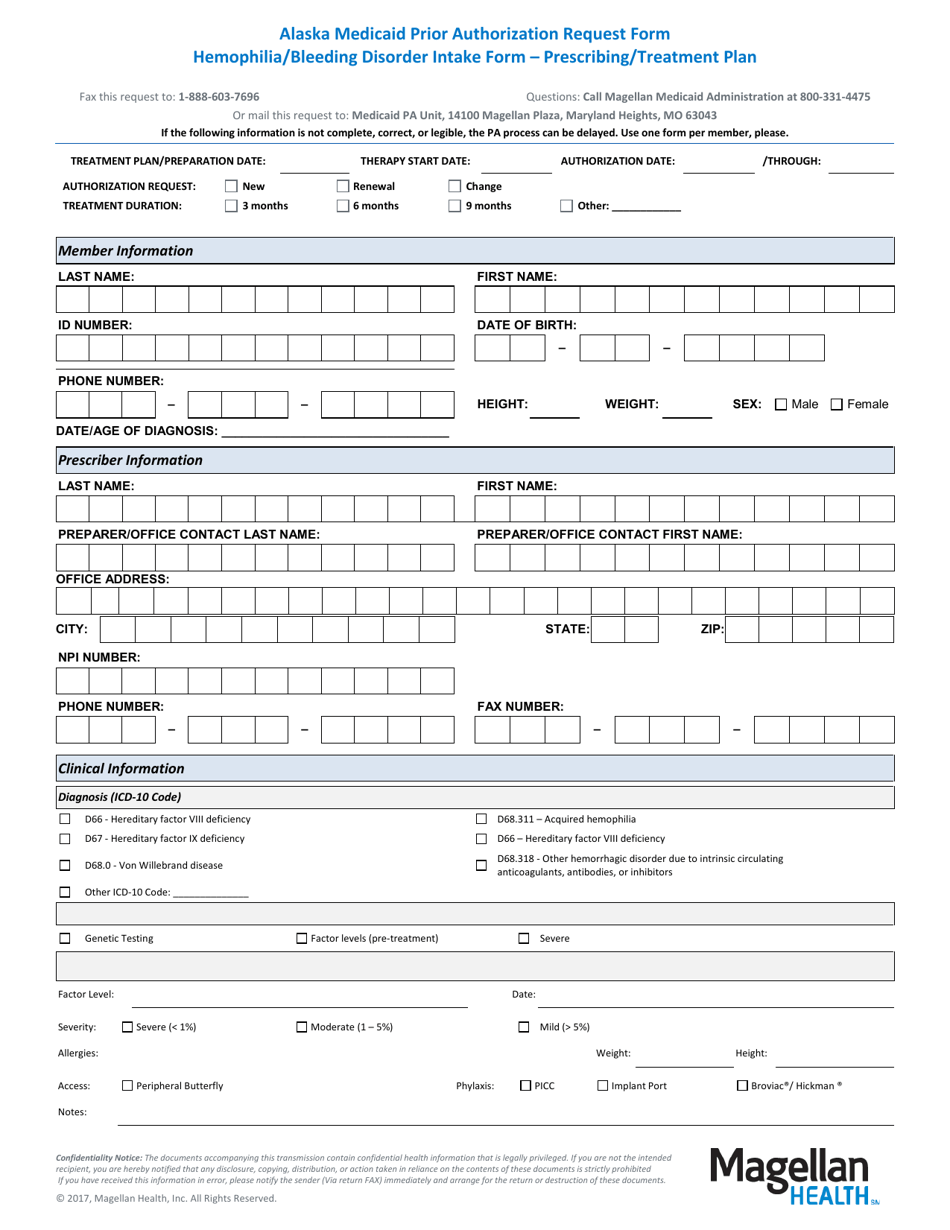
Alaska Medicaid Prior Authorization Request Form - Hemophilia / Bleeding Disorder Intake Form - Prescribing / Treatment Plan - Alaska

Alaska Medicaid Prior Authorization Request Form - Hemophilia/Bleeding Disorder Intake Form - Prescribing/Treatment Plan is a legal document that was released by the Alaska Department of Health and Social Services - a government authority operating within Alaska.
FAQ
Q: What is the Alaska Medicaid Prior Authorization Request Form?
A: It is a form used for requesting prior authorization for Medicaid services in Alaska.
Q: What is the Hemophilia/Bleeding Disorder Intake Form?
A: It is a form used to gather information about patients with hemophilia or bleeding disorders.
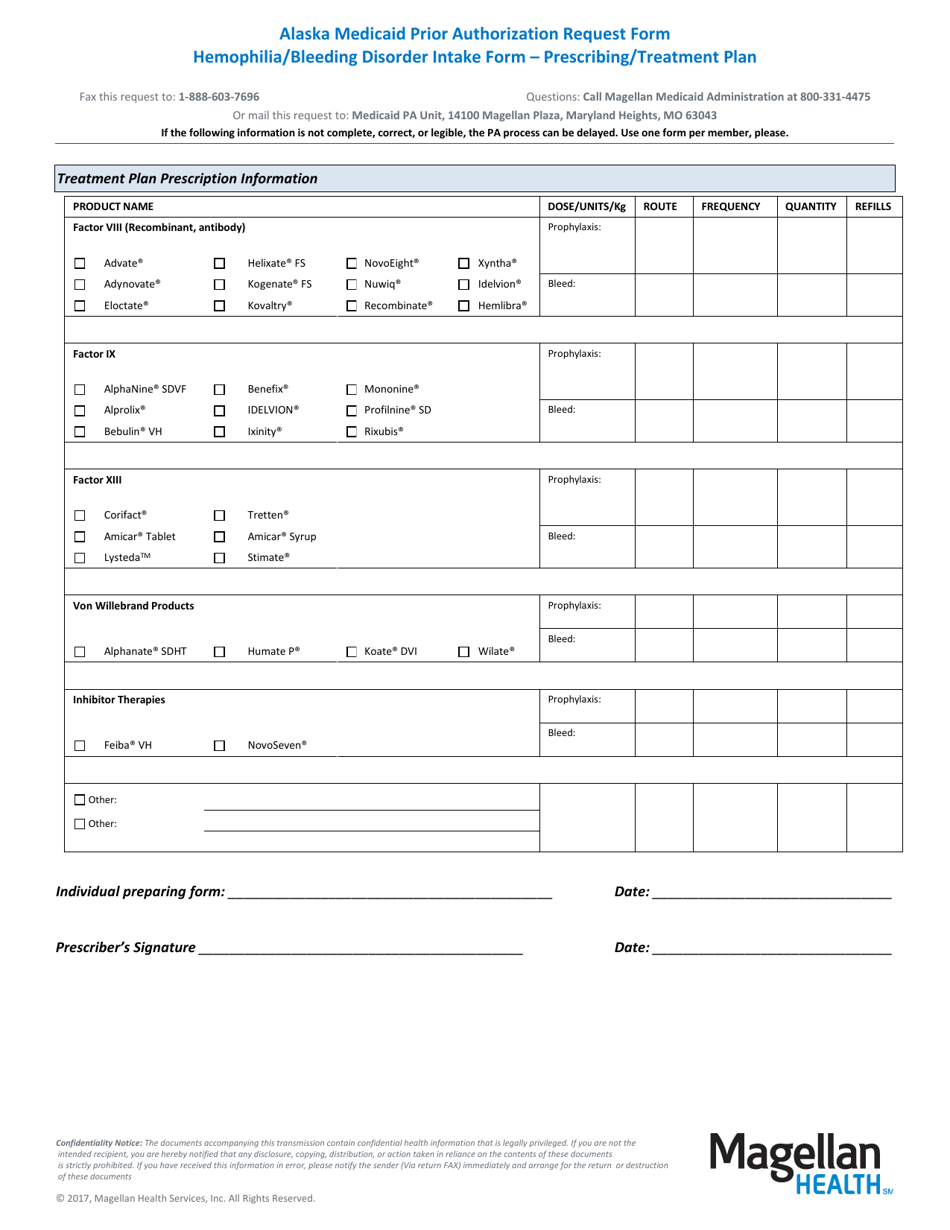
Q: What is the purpose of the Prescribing/Treatment Plan form?
A: It is used to outline the recommended medications and treatments for patients with hemophilia or bleeding disorders in Alaska.
Q: Who should use these forms?
A: Healthcare providers in Alaska who are treating patients with hemophilia or bleeding disorders and need to request prior authorization for Medicaid services.
Q: Why is prior authorization necessary?
A: Prior authorization is required by Alaska Medicaid to ensure that the requested services and treatments are medically necessary and appropriate.
Form Details:
- The latest edition currently provided by the Alaska Department of Health and Social Services;
- Ready to use and print;
- Easy to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of the form by clicking the link below or browse more documents and templates provided by the Alaska Department of Health and Social Services.
Download Alaska Medicaid Prior Authorization Request Form - Hemophilia / Bleeding Disorder Intake Form - Prescribing / Treatment Plan - Alaska
1
2