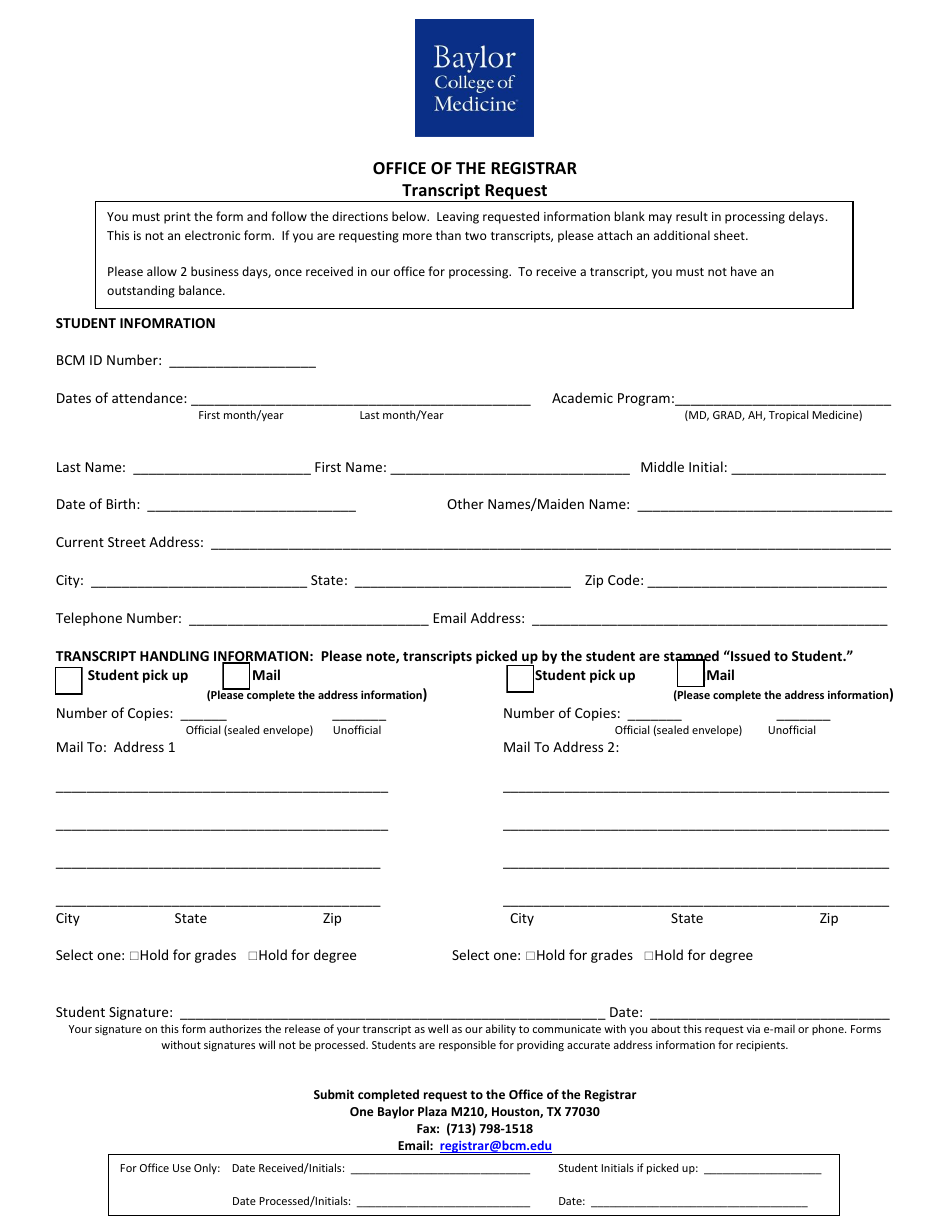
Transcript Request Form - Baylor College of Medicine - Houston, Texas
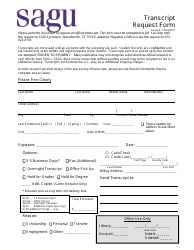
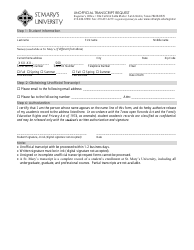
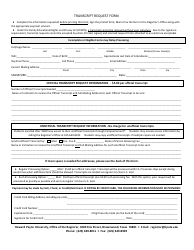
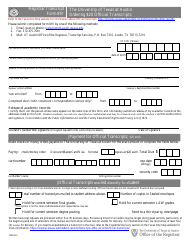
The Transcript Request Form from Baylor College of Medicine in Houston, Texas is used to request official transcripts of academic records from the college.
The student or applicant typically files the transcript request form at Baylor College of Medicine in Houston, Texas.
FAQ
Q: How do I request a transcript from Baylor College of Medicine?
A: You need to fill out the Transcript Request Form and submit it to the college.
Q: What is the address of Baylor College of Medicine in Houston, Texas?
A: The address is 1 Baylor Plaza, Houston, Texas.
Q: How long does it take to process a transcript request?
A: The processing time for a transcript request varies, but it typically takes a few business days.
Q: Is there a fee for requesting a transcript?
A: Yes, there is usually a fee associated with requesting a transcript.