Form DOH-694 Hospital and Community Patient Review Instrument (Hc-Pri) - New York
What Is Form DOH-694?
This is a legal form that was released by the New York State Department of Health - a government authority operating within New York. As of today, no separate filing guidelines for the form are provided by the issuing department.
FAQ
Q: What is the DOH-694 form?
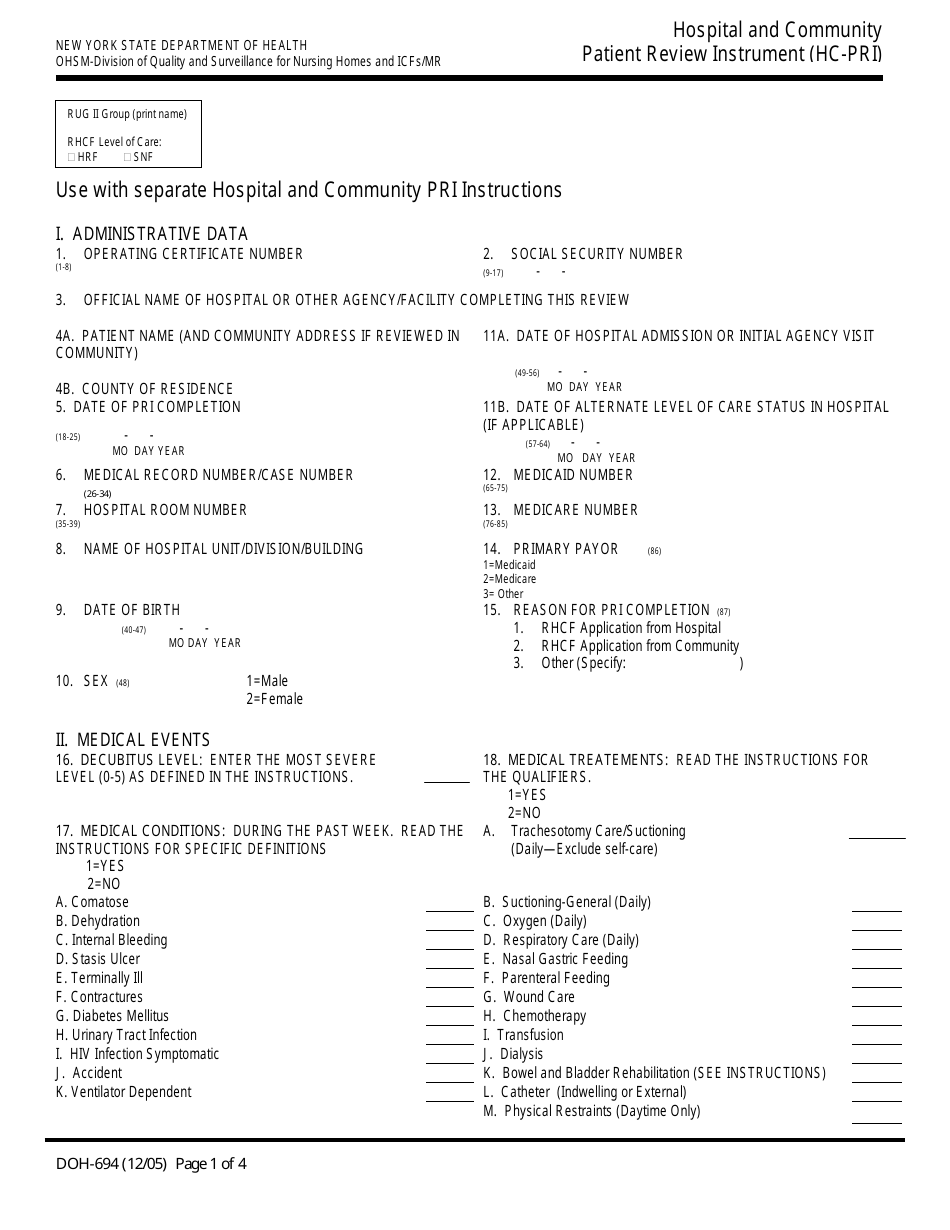
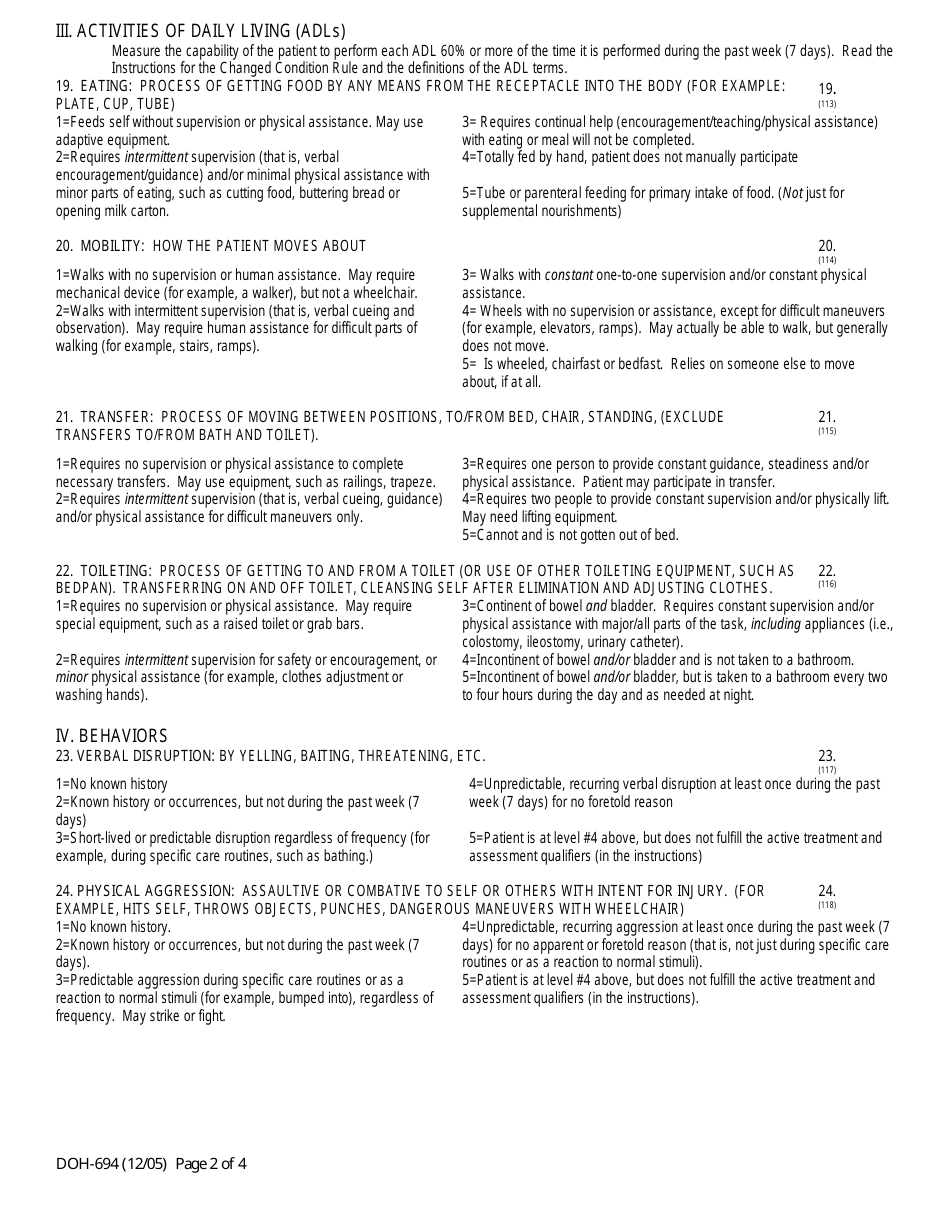
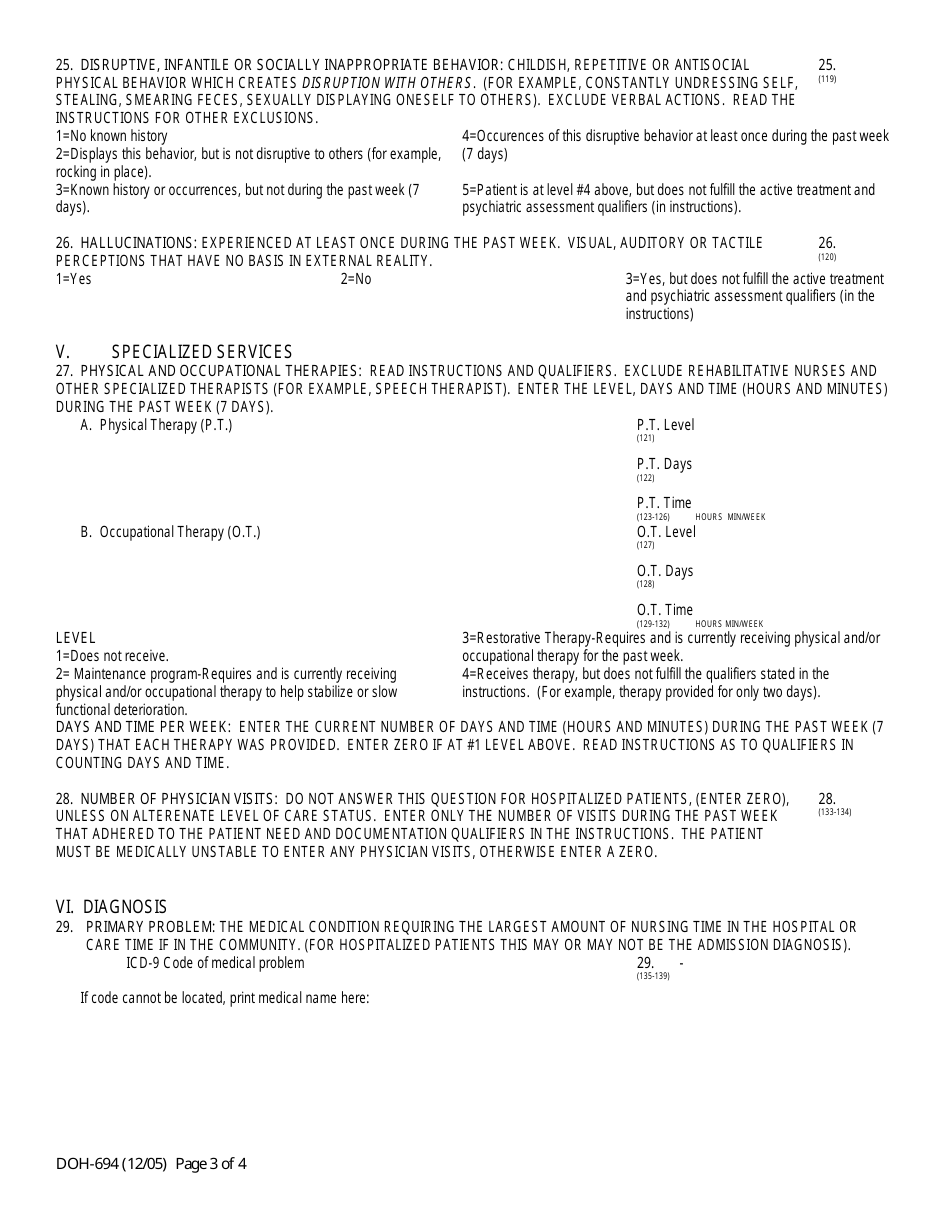
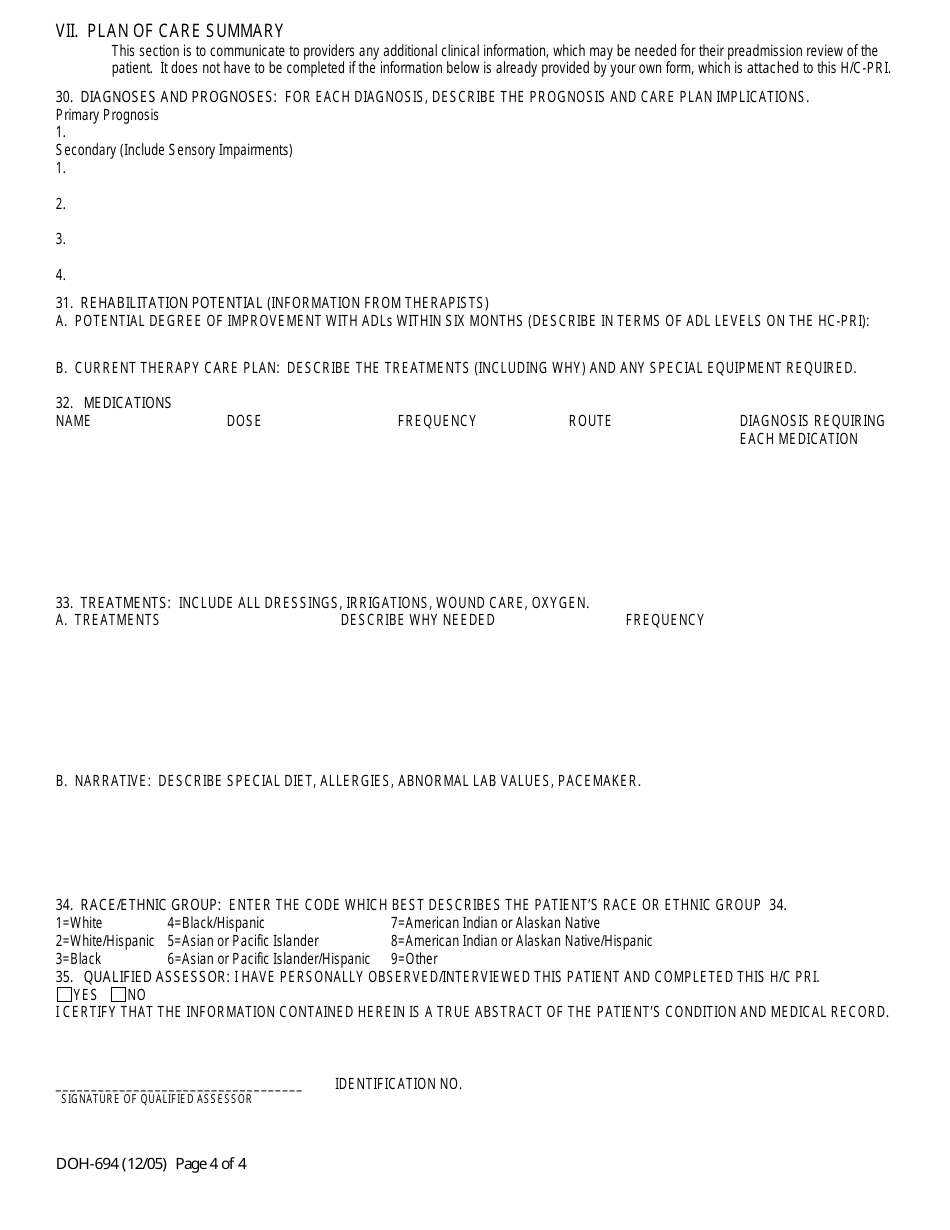
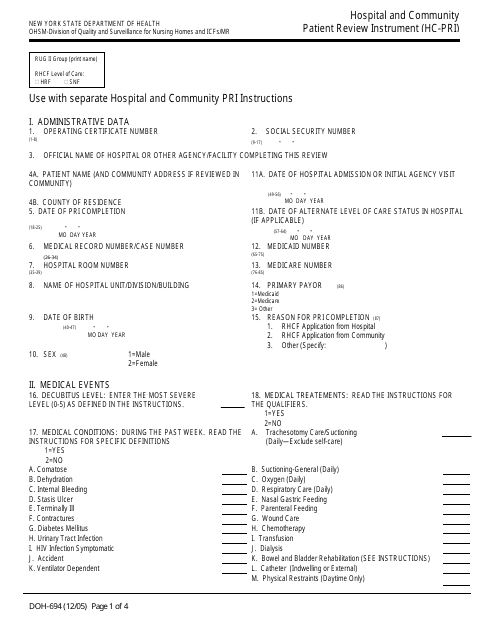
A: The DOH-694 form is the Hospital and Community Patient Review Instrument (Hc-Pri) used in New York.
Q: What is the purpose of the DOH-694 form?
A: The purpose of the DOH-694 form is to conduct assessments of patients in hospitals and the community to determine eligibility for certain health care services.
Q: Who uses the DOH-694 form?
A: The DOH-694 form is used by health care providers and facilities in New York.
Q: What information is collected on the DOH-694 form?
A: The DOH-694 form collects information about the patient's medical conditions, functional abilities, and support needs.
Q: What is the importance of the DOH-694 form?
A: The DOH-694 form is important for determining eligibility for certain health care services and ensuring appropriate care for patients in New York.
Form Details:
- Released on December 1, 2005;
- The latest edition provided by the New York State Department of Health;
- Easy to use and ready to print;
- Quick to customize;
- Compatible with most PDF-viewing applications;
- Fill out the form in our online filing application.
Download a printable version of Form DOH-694 by clicking the link below or browse more documents and templates provided by the New York State Department of Health.
Download Form DOH-694 Hospital and Community Patient Review Instrument (Hc-Pri) - New York

1

2

3

4