Fill and Sign Legal Forms and Templates
Documents:
152222
This form is used for requesting a temporary Continuing Education (CE) waiver in California due to a disability or medical condition.
This Form is used for notifying the California Department of Consumer Affairs (DCA) of address changes.
This form is used for submitting a quarterly report to the California Department of Consumer Affairs. It is necessary for businesses operating in California to provide this report detailing their activities and financial information for the specified quarter.
This document is used for certifying an out-of-state degree program for professional clinical counselors in California.
This Form is used for obtaining certification as an Associate Marriage and Family Therapist in California.
This document is for obtaining certification as an Associate Marriage and Family Therapist in California. It is used to certify completion of an in-state degree program.
This Form is used for applying to become a provider of continuing education in Florida.
This Form is used for applying for course approval for continuing education in the state of Florida.
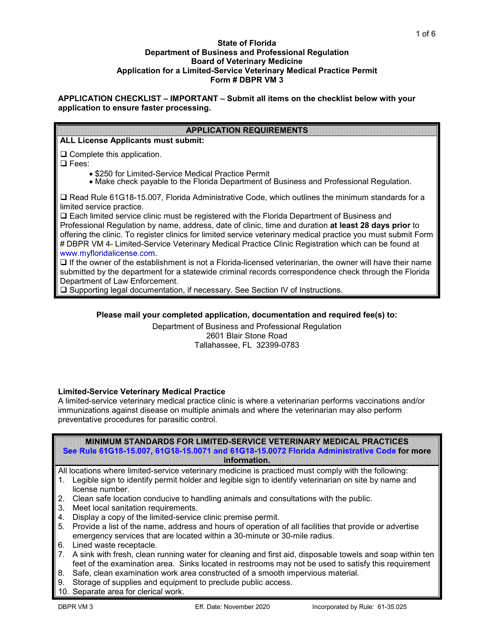
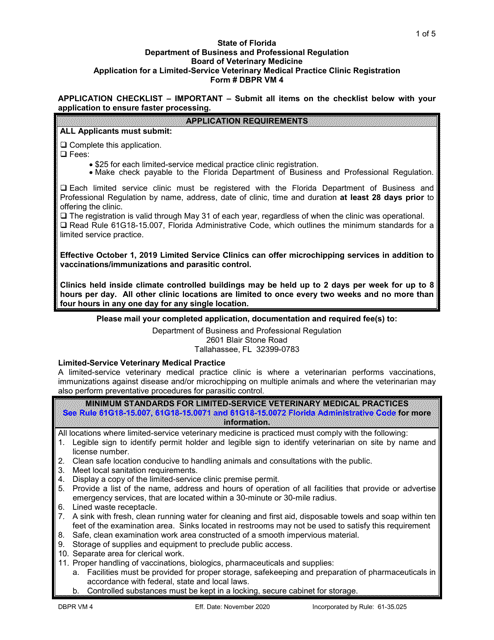
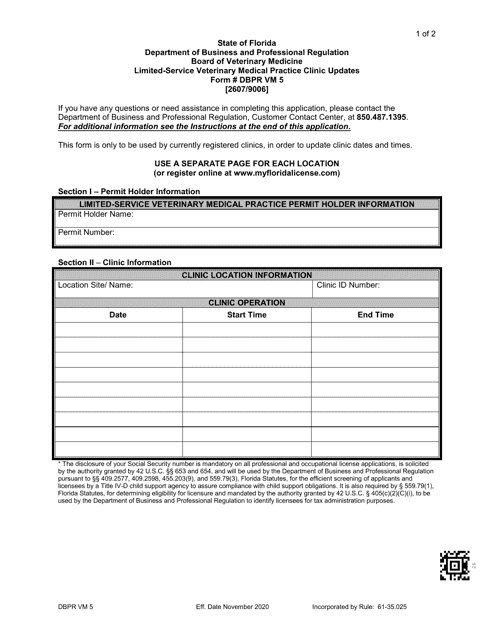
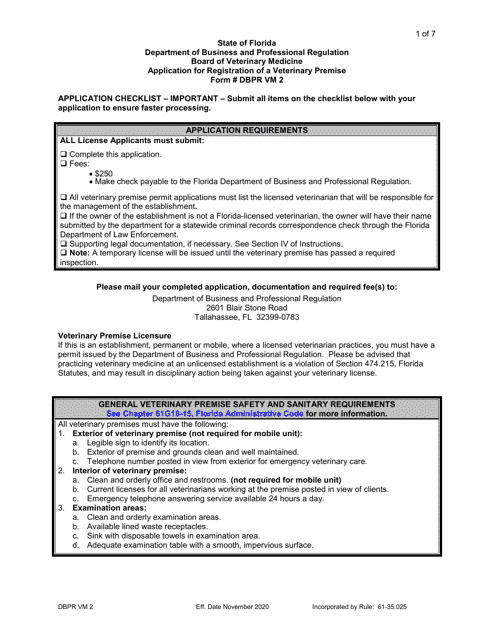
This form is used for changing the name of a veterinary premise or clinic in the state of Florida.

This form is used for making corrections to prior authorizations in the Tribal Health Program in Arizona.
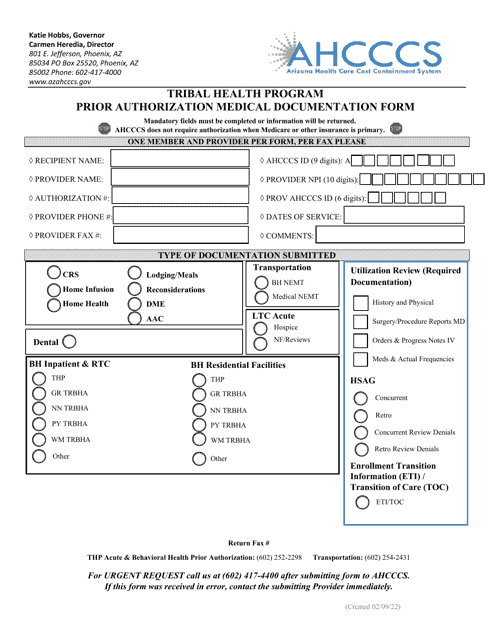
This Form is used for submitting medical documentation for prior authorization through the Tribal Health Program in Arizona.
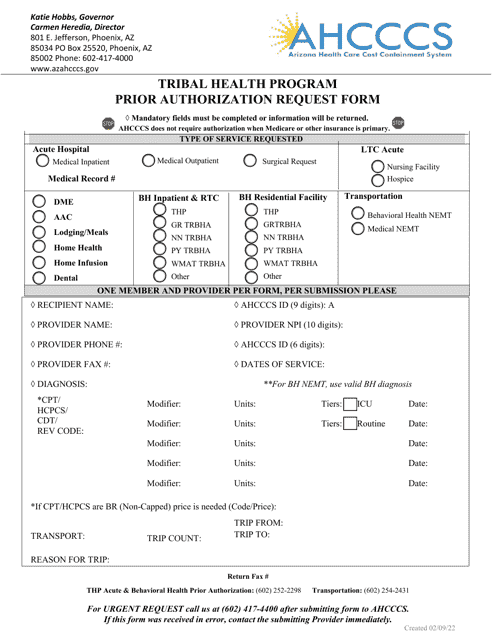
This form is used to request prior authorization for medical services under the Tribal Health Program in Arizona.
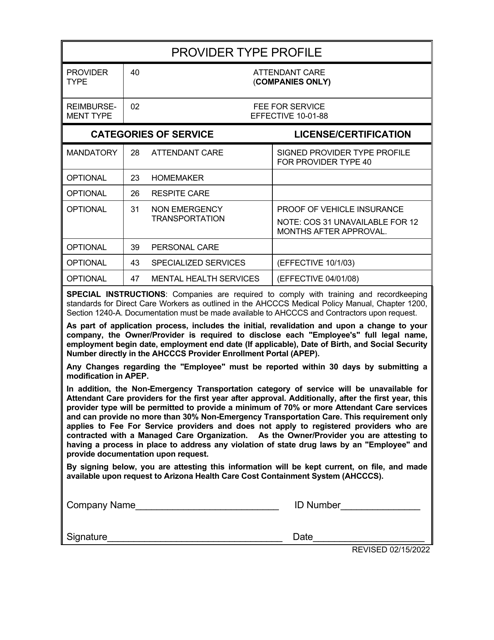
This type of document provides a profile for companies offering attendant care services in Arizona. It includes information about the company's background, services provided, and contact details.
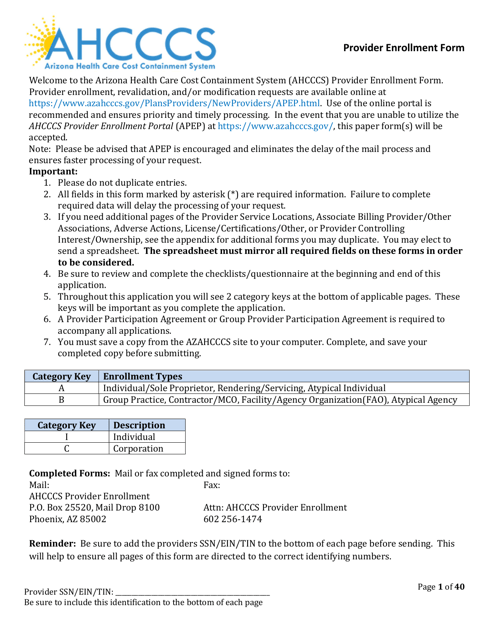
This Form is used for enrolling healthcare providers in the state of Arizona. It is the official document required for providers to participate in state healthcare programs and receive reimbursement for services provided.
This form is used for requesting information for victims of crimes in Nova Scotia, Canada.
This type of document is used to authorize the release of protected medical information to Ahcccs in Arizona.
This Form is used for authorizing Ahcccs to disclose protected health information about your health in Arizona. This document is in Spanish and has large font.
This type of document is an affirmation statement for external users of the Arizona Health Care Cost Containment System (AHCCCS).
This form is used for submitting a request to the American Indian Medical Home in Arizona. It serves as a cover sheet for faxing the application.
This form is used for new members to sign up for the American Indian Medical Home program in Arizona.
This document is a sign-up form for American Indian individuals who wish to become members of the Medical Home program in Arizona. The form is available in Spanish.
