Mississippi Division of Medicaid Forms
Documents:
105
This form is used to appoint an authorized representative or agent for a provider in the state of Mississippi.
This form is used for requesting medical supplies under fee-for-service in the state of Mississippi. It certifies the medical necessity of the supplies being requested.
This document is used for enrolling private duty nursing and personal care service providers in Mississippi's State Plan Supplemental Program.
This document is for certifying the medical necessity of non-emergency ambulance transportation between hospitals in Mississippi. It ensures that the patient requires transportation by ambulance and is not able to use other means of transportation.
This document is for a survey conducted in Mississippi to gather information from Mississippican and chip providers.
This document is a Provider Agreement for Early and Periodic Screening, Diagnosis, and Treatment (EPSDT) in Mississippi. It outlines the agreement between the provider and the state for delivering comprehensive healthcare services to eligible children.
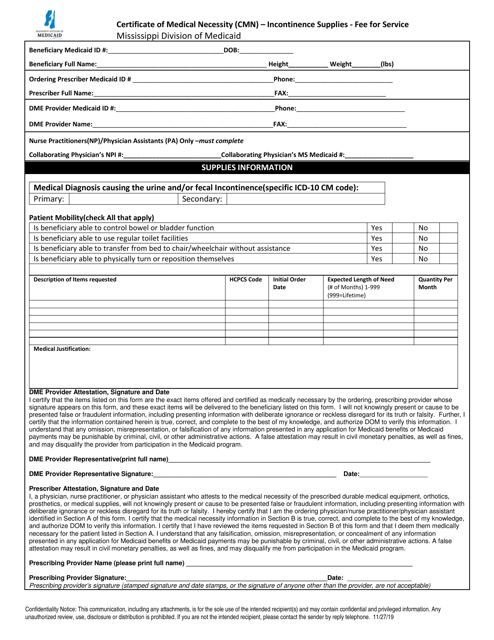
This document is for obtaining reimbursement for incontinence supplies in Mississippi under fee-for-service healthcare. A Certificate of Medical Necessity (CMN) is required to demonstrate the need for these supplies.
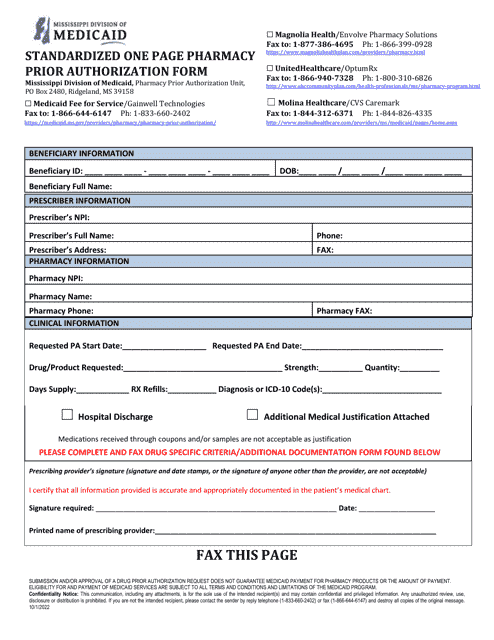
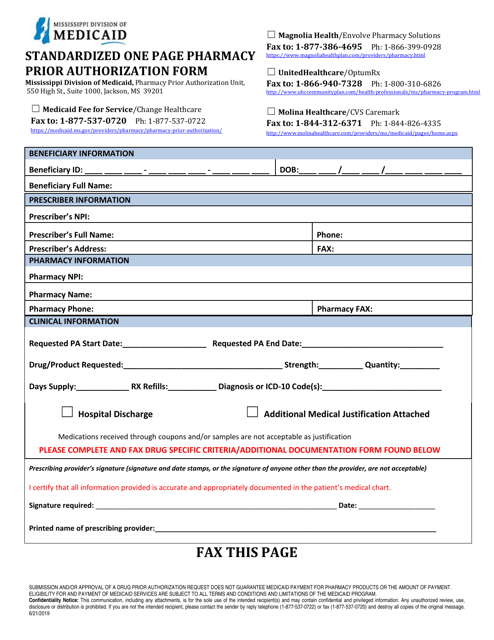
This type of document is a standardized one-page form used in Mississippi for the prior authorization of human growth hormone medication in pharmacies.
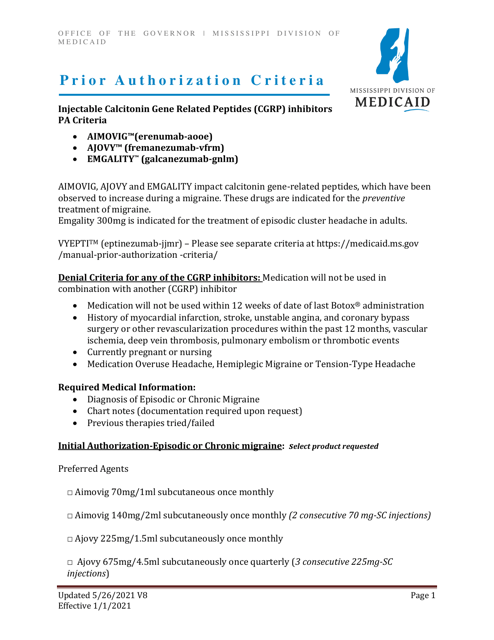
This document outlines the criteria for obtaining prior authorization for Injectable Calcitonin Gene Related Peptides (CGRP) inhibitors in the state of Mississippi.
This document outlines the criteria that must be met for obtaining prior authorization for the medication Evrysdi (Risdiplam) in the state of Mississippi. It specifies the requirements that must be met in order for the medication to be approved for coverage.
This type of document provides the criteria for obtaining prior authorization for the medication Eteplirsen, also known as Exondys 51, in the state of Mississippi.
This document outlines the criteria required for obtaining prior authorization for the medication Viltepso (Viltolarsen) in the state of Mississippi.
This type of document outlines the criteria that must be met for obtaining prior authorization for the medication Vyondys 53 (Golodirsen) in the state of Mississippi. It provides guidelines for determining eligibility for coverage.
This Form is used for filing a B Election Notice in the state of Mississippi.
This form is used for notifying hospice election or discharge for dual eligible beneficiaries in Mississippi.
This document is used for establishing an agreement and enrollment between healthcare providers and the Mississippi Electronic Data Interchange (EDI) system.
This document is a request for information related to civil rights compliance for Medicaid certification in the state of Mississippi.
This Form is used for disclosing information about providers participating in Mississippi Medicaid program. It ensures transparency and accountability in the healthcare system.
This document is a cover letter that accompanies an application for an out-of-state provider to practice in the state of Mississippi.
This document is a Data Use Agreement specific to the state of Mississippi. It outlines how data will be used, shared, and protected in accordance with state regulations.
This form is used for attaching additional documents or evidence to support a claim in the state of Mississippi.
This type of document is used for requesting prior authorization for EPSDT (Early and Periodic Screening, Diagnostic, and Treatment) services for beneficiaries under 21 years old in Mississippi.
This type of document is a Prior Authorization Packet specifically for Growth Hormone medications in the state of Mississippi. It is used to request approval from the insurance company for coverage of these medications.
This document is used for obtaining prior authorization for opioids in the state of Mississippi. It includes the necessary paperwork and information required to request approval for the use of these medications.
This document provides the specific criteria and guidelines for obtaining prior authorization for the medication Dupixent for the treatment of Prurigo Nodularis in the state of Mississippi.
This document is used for requesting approval for a maximum unit override for healthcare services in the state of Mississippi. It allows healthcare providers to exceed the usual limits set by insurance companies for the number of units of a specific service that can be provided.