Prior Authorization Request Form Templates
Documents:
132
This form is used for requesting prior authorization for pulmonary arterial hypertension agents in Nevada.
This Form is used for requesting prior authorization for Xyosted in the state of Nevada.
This form is used for requesting prior authorization for oral oncology agents in the state of Nevada.
This form is used for requesting prior authorization for immunomodulator drugs in the state of Nevada.
This form is used for requesting prior authorization for the medication Linezolid (brand name Zyvox) in the state of Nevada.
This Form is used for requesting prior authorization for the medication Elidel (Pimecrolimus) in Nevada.
This document is a Prior Authorization Request Form for the medication Protopic (Tacrolimus) in the state of Nevada. It is used to seek approval from the healthcare provider or insurance company for coverage of this medication.
This form is used for requesting prior authorization for Eucrisa medication in Nevada.
This Form is used for requesting prior authorization for the medication Daliresp in the state of Nevada.
This form is used for submitting a prior authorization request for Zolgensma medication in the state of Nevada. The form is used to seek approval for coverage of this specific medication.
This Form is used for requesting prior authorization for Continuous Glucose Monitors (CGMs) in the state of Nevada.
This form is used for requesting prior authorization for insulin pump coverage in Nevada.
This Form is used for requesting prior authorization for hematopoietic/hematinic agents in Nevada.
This Form is used for requesting prior authorization for Nayzilam in the state of Nevada.
This Form is used for requesting prior authorization for the medication Wakix (Pitolisant) in Nevada.
This document is a prior authorization request form for Toradol (Ketorolac Tromethamine), a medication used for pain relief. It is specifically for residents in Nevada.
This form is used for requesting prior authorization for bid dosing of PPI medication in Alaska.

This form is used for requesting prior authorization for Medicaid coverage in Alaska specifically for the treatment of hemophilia or bleeding disorders. It includes an intake form and a prescribing/treatment plan.
This Form is used to request prior authorization for antihemophilia agents in Nevada. It helps ensure that patients receive the necessary medications for treating hemophilia.
This form is used for requesting prior authorization for Exondys 51 medication in the state of Nevada.
This Form is used for requesting prior authorization for the medication called Somavert (Pegvisomant) in the state of Nevada.
This form is used for requesting prior authorization for durable medical equipment in South Dakota.
This form is used for requesting prior authorization for medical nutrition services in South Dakota.
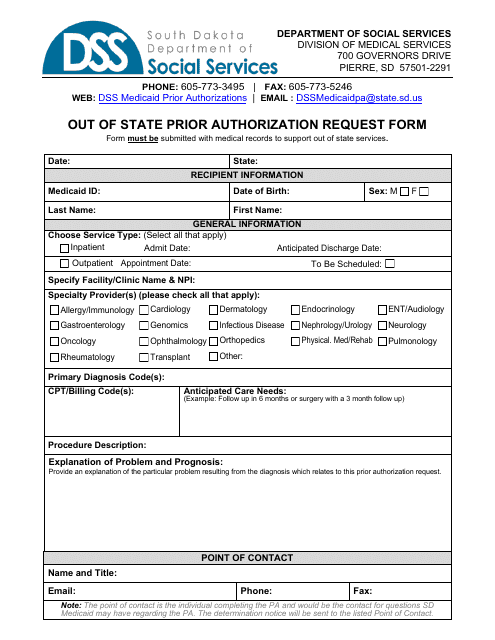
This form is used for requesting prior authorization for long term acute care or out-of-state rehab services in South Dakota.
This Form is used for requesting prior authorization for the medication Tymlos (Abaloparatide) in Nevada.
This Form is used for requesting prior authorization for the medication Orilissa (Elagolix) in the state of Nevada.
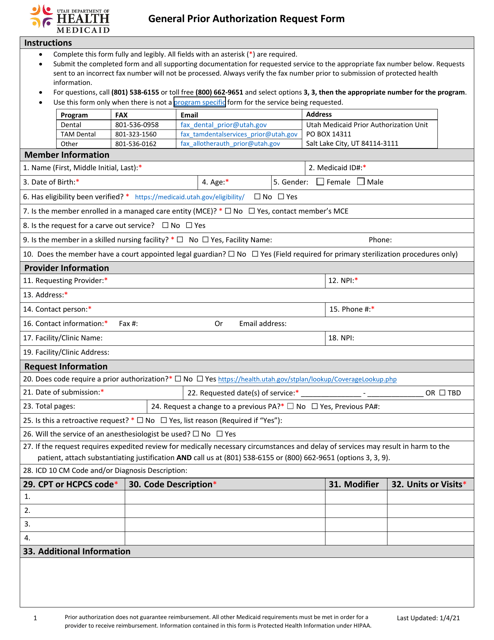
This Form is used for requesting prior authorization for medical services or treatments in the state of Utah. It helps ensure that the requested service is medically necessary and covered by the insurance provider.
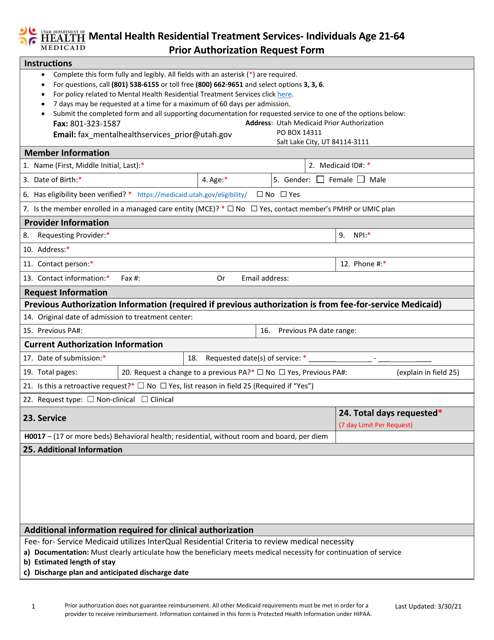
This form is used for requesting prior authorization for mental health residential treatment services for individuals aged 21-64 in Utah.
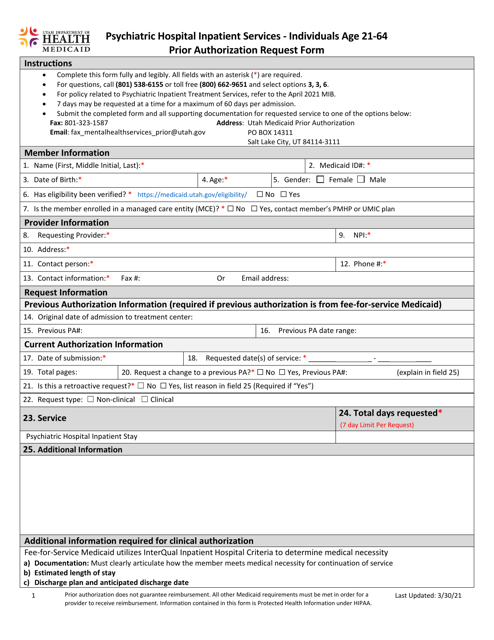
This form is used for requesting prior authorization for individuals aged 21-64 who require psychiatric hospital inpatient services in the state of Utah. It helps ensure that the necessary care and treatment are provided to patients in need.
This type of document is a questionnaire used to request prior authorization for a Cpap or BI-Level (Pap) machine in the state of Colorado.
This Form is used for requesting prior authorization of Evrysdi (Risdiplam) medication in Nevada.
