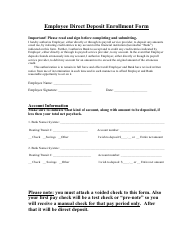
Employee Direct Deposit Enrollment Form - Basic Flex
The Employee Direct Deposit Enrollment Form - Basic Flex is used for enrolling in direct deposit, which allows employees to have their paychecks automatically deposited into their bank accounts.
The employee themselves typically files the Employee Direct Deposit Enrollment Form - Basic Flex.
FAQ
Q: What is the Employee Direct Deposit Enrollment Form?
A: It is a form to enroll in direct deposit for employee paychecks.
Q: What is direct deposit?
A: Direct deposit is a safe and convenient way to receive your paycheck electronically into your bank account.
Q: Why should I enroll in direct deposit?
A: Enrolling in direct deposit saves time and eliminates the need to physically deposit your paycheck.
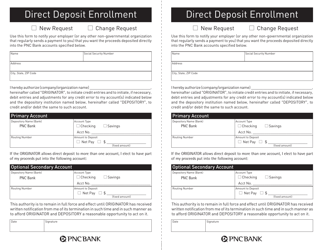
Q: Can I choose which bank account to use for direct deposit?
A: Yes, you can select the bank account where you want your paycheck deposited.
Q: Are there any fees for direct deposit?
A: Most employers offer direct deposit for free, but it's best to check with your employer to confirm.
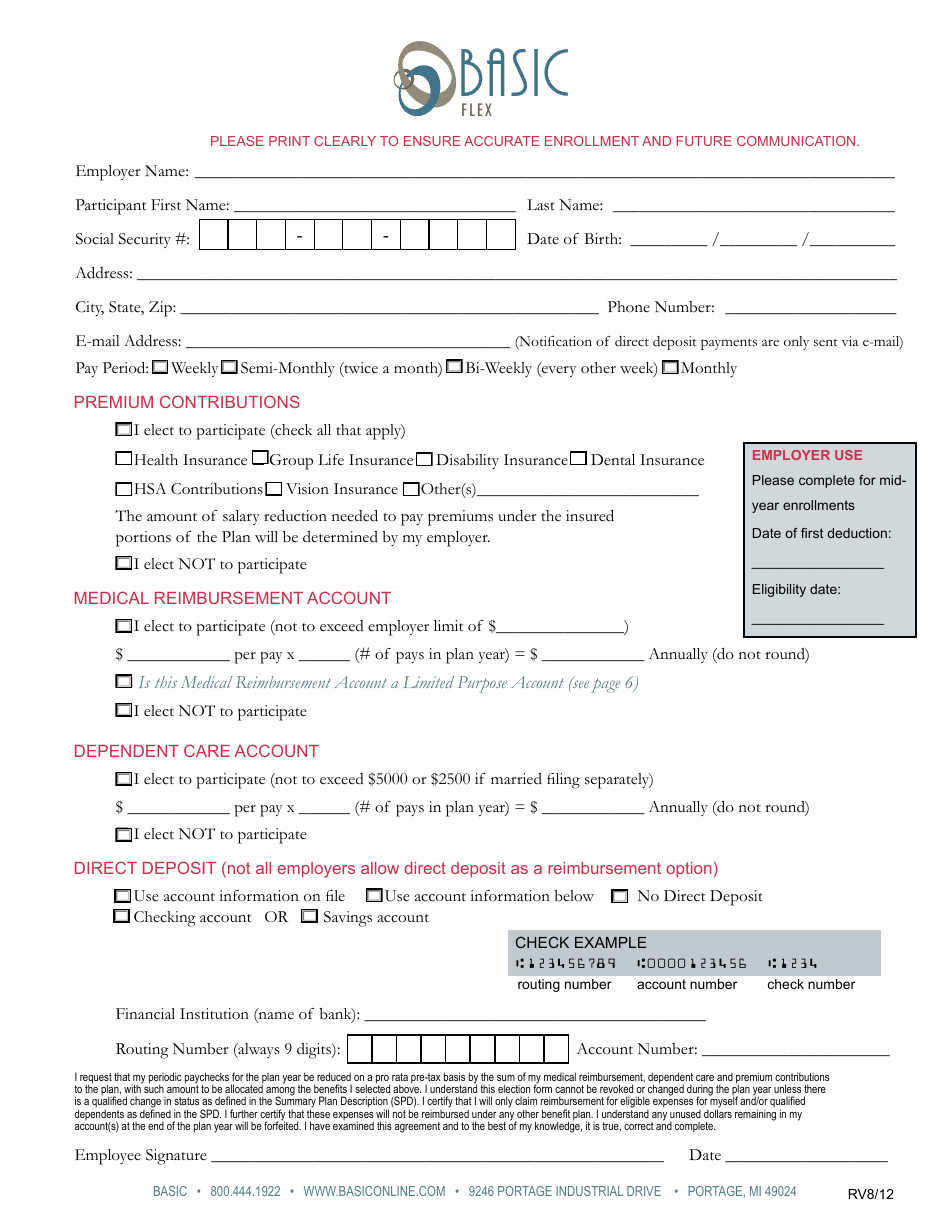
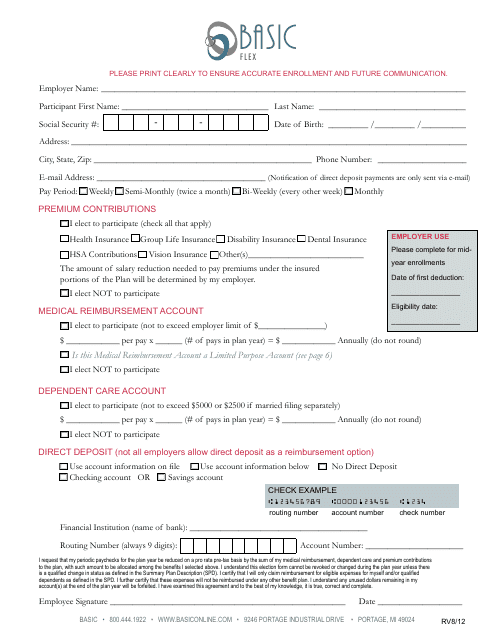
Q: How do I fill out the Employee Direct Deposit Enrollment Form?
A: You need to provide your personal information, bank account details, and sign the form.
Q: Who should I submit the form to?
A: Submit the completed form to your employer's HR or payroll department.
Q: When will direct deposit take effect?
A: Direct deposit usually takes effect within one to two pay periods after submitting the form.
Q: Can I cancel or change my direct deposit information?
A: Yes, you can cancel or update your direct deposit by submitting a new form to your employer.
Q: Is direct deposit available for all types of payments?
A: Direct deposit is commonly used for payroll payments, but availability may vary for other types of payments.