Occupational Injury Templates
Are you dealing with occupational injuries at your workplace? Our website provides a comprehensive collection of documents relating to occupational injuries to help you navigate through the administrative processes smoothly. From supervisor's reports to injury recurrence notices, we have all the necessary forms to ensure proper documentation of your occupational injury. Our library includes various forms such as Form CA-2A Notice of Recurrence, Form HUD-795 Supervisor's Report of Occupational Injury, Illness, Accident or Fire, and Form D-9A Permanent Partial Disability Award Calculation Worksheet - Nevada, among others. Whether you are an employee or a supervisor, our documents will assist you in effectively reporting, reviewing, and managing occupational injuries. With our user-friendly website, you can easily access and download the required forms to stay compliant with the necessary legal and administrative procedures. Browse through our collection of occupational injury documents and gain peace of mind knowing that you have the right tools to address any occupational injury situation.
Documents:
59
This document is used for reporting the first injury of an employee to their supervisor at Bentley University.
This form is used for reporting occupational injuries or illnesses by doctors in California.
This document is used for reporting accidents and documenting the details of the incident. It helps gather important information necessary for insurance claims and legal purposes.
This form is used for employers in Connecticut to report any job-related injuries or illnesses that occur in their workplace. It ensures that the appropriate authorities are aware of the incident and allows for workers' compensation benefits to be provided if necessary.
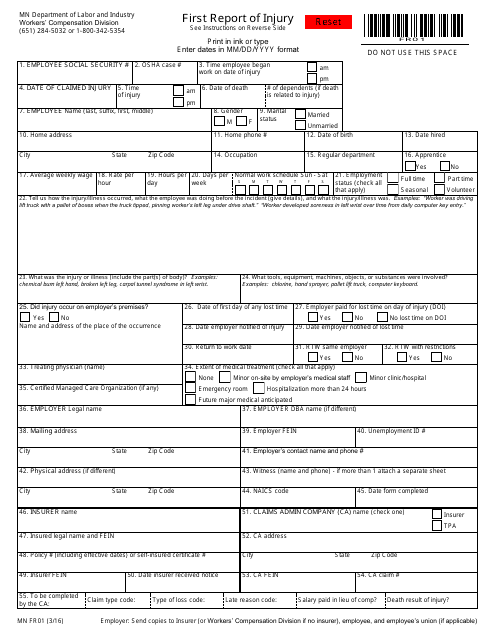
This form is used for reporting the first injury that occurs in the workplace in the state of Minnesota. It is important to fill out this form to ensure that the appropriate actions are taken to support the employee and prevent future injuries.
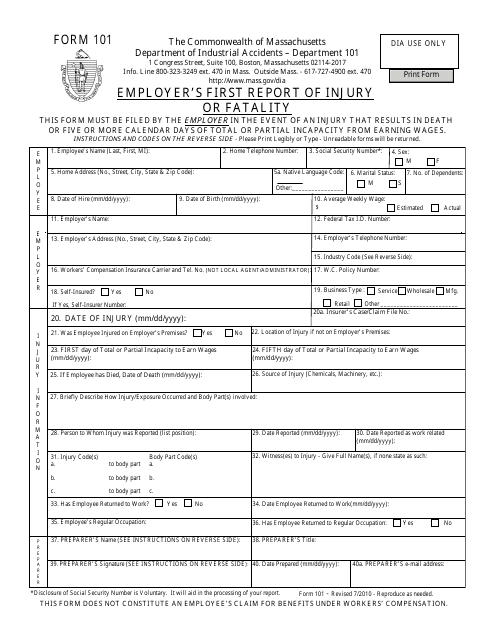
This form is used for employers in Massachusetts to report any work-related injuries or fatalities to the state authorities.
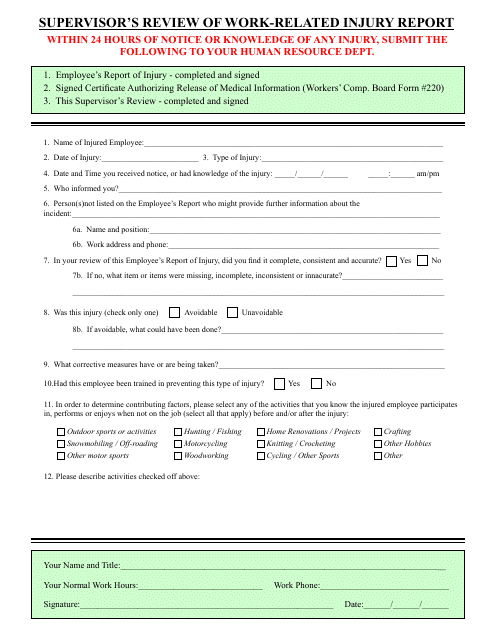
This document is for the supervisor to review a report related to work-related injuries. It is used to assess the details of the incident and determine any necessary actions.
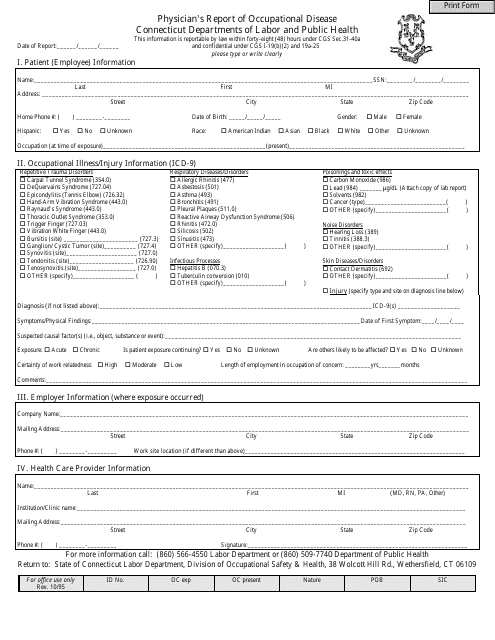
This form is used to report occupational diseases in Connecticut, providing details about the patient's condition and its relation to their work environment.
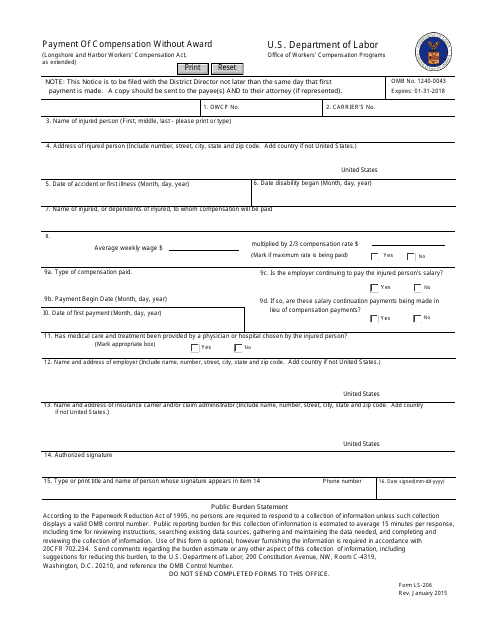
This form is used for requesting the payment of compensation to an employee without a formal award.
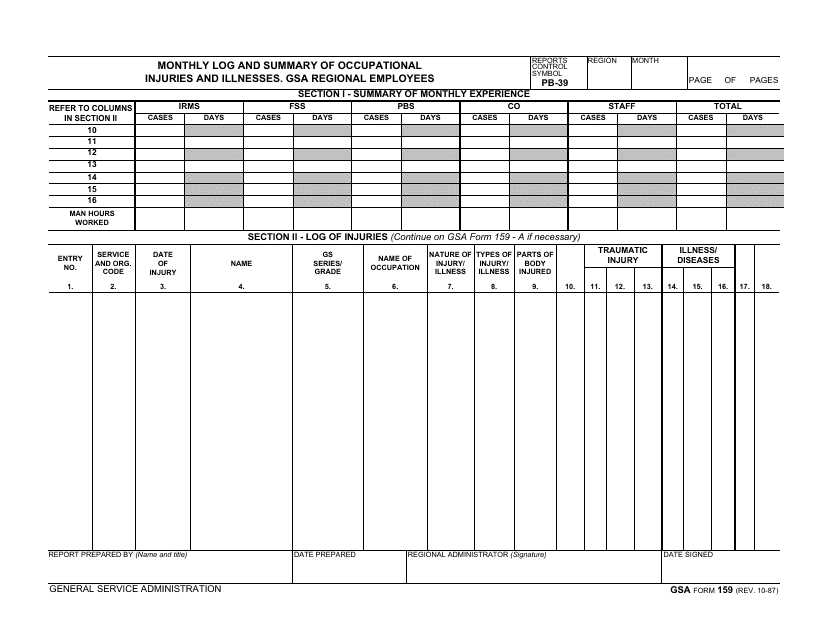
This Form is used for recording and summarizing the occupational injuries and illnesses of GSA regional employees on a monthly basis.
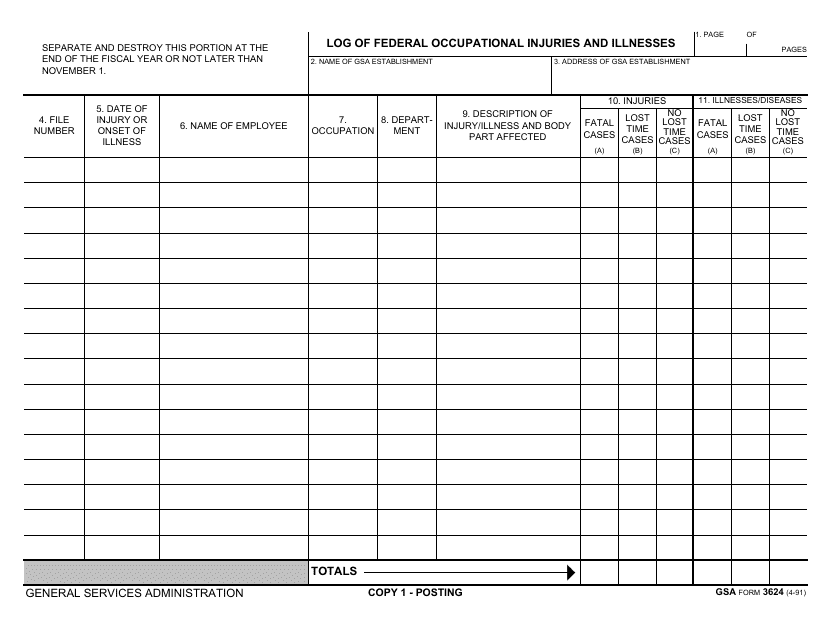
This Form is used for logging and tracking federal occupational injuries and illnesses.
This Form is used for employers in Alaska to provide notice of 90 consecutive days of time loss for injuries suffered by an employee. It is important for employers to fill out this form accurately and submit it to the appropriate authorities.
This document is used for filing a supplemental claim for compensation for workers in the state of Arizona. It allows workers to request additional compensation for work-related injuries or illnesses.
This form is used for reporting the first occurrence of an injury or illness in the state of Florida. It is important to complete and submit this form as soon as possible after the incident.
This form is used for workers in Nevada who need to indicate their choice of leave for workers' compensation purposes.
This Form is used for reporting employee injuries or illnesses that occur in the state of Michigan. It helps employers comply with state regulations and keep a record of workplace incidents.
This document outlines the rights and responsibilities of an injured worker in Minnesota regarding rehabilitation. It is used for understanding the entitlements and obligations of injured workers during the rehabilitation process.
This form is used for applying for membership in Missouri.
This document is for employers in New York to report work-related injuries or illnesses in Haitian Creole. It is used to provide necessary information about the incident.
This document is used for submitting an Ancillary Medical Report in New York State. It is used to provide additional medical information related to a worker's compensation claim.
This form is used for requesting salary continuation or extending/reactivating occupational injury leave in Ohio.
This Form is used for employers in Vermont to report the first injury or illness that occurs on the job.
This Form is used for providing workers' compensation information in Pennsylvania.

This form is used for employers in New Hampshire to report the first injury that has occurred in the workplace.
This form is used for primary treating physicians in California to report on the permanent and stationary status of the injured worker.
This form is used for Chinese employees in New York to file a claim for various employment-related matters.
This form is used for California employers to report occupational injuries or illnesses suffered by their employees.
This form is used for reporting the first occurrence of an occupational injury or illness in California. It is filled out by the doctor to provide detailed information about the incident, including the nature of the injury or illness, its cause, and the treatment provided.
This document is used for reporting chiropractic or acupuncture personal injuries in California.
This form is used for reporting a supplemental report of a fatal injury in the state of Michigan.
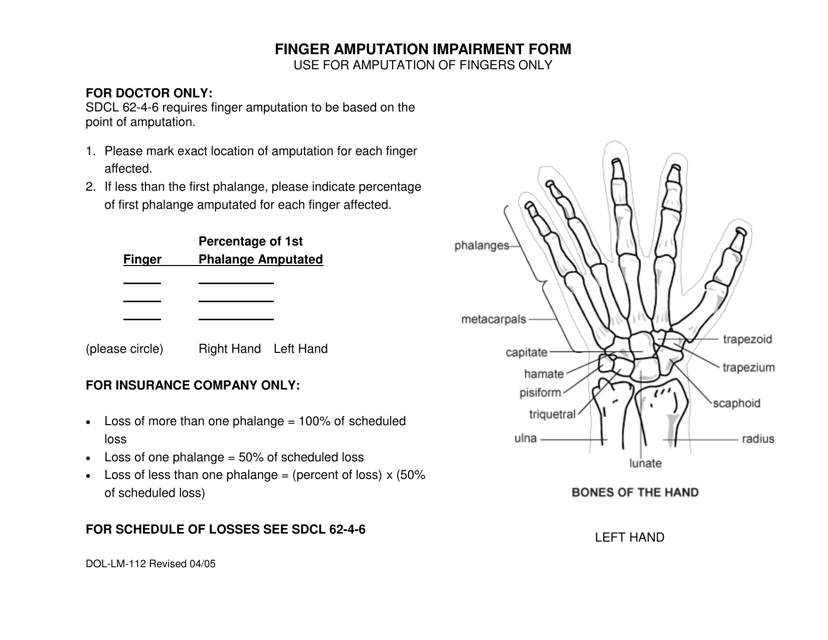
This document is for reporting finger amputation impairment in South Dakota. It is used to provide relevant information about the amputation to the Department of Labor in order to assess disability benefits.
